 EN
EN FR
FR
by A Midwestern Doctor,
Why a single agent, through its forgotten biophysical effects, can reverse an improbable range of “incurable” neurological conditions.
Story at a Glance:
- DMSO is an “umbrella remedy” whose combination of therapeutic properties (improving circulation, reducing inflammation, protecting cells, and reviving dying ones) makes it uniquely suited to treat a variety of conditions, particularly “incurable” neurological disorders and the chronic pain that accompanies them.
- Through its actions on water, DMSO temporarily shifts the phase of cell membranes and cytoskeletons, after which they reform in a strengthened configuration, facilitating DMSO’s prized ability to transport substances across biological barriers without damaging them and creating a cellular reset that can resolve dysfunctional circuits giving rise to a variety of neurological disorders.
- DMSO selectively blocks the small nerve fibers responsible for chronic pain transmission while not affecting larger fibers, safely eliminating pain other medications cannot reduce. Hundreds of readers have reported it transforming chronic neuropathic pain, migraines, fibromyalgia, and nerve damage from diabetes, chemotherapy, vaccines, and surgery, often after years of failed conventional treatments.
- DMSO promotes peripheral nerve regeneration and addresses the root causes of pain through multiple converging mechanisms, with readers reporting return of sensation and motor function in nerves damaged for years or even decades.
- DMSO has been extensively used in clinical practice for peripheral neuropathies, with Level 1 evidence for complex regional pain syndrome (CRPS) and demonstrated benefit for facial nerve palsy, trigeminal neuralgia, post-herpetic neuralgia, compression neuropathies, diabetic neuropathy, and fibromyalgia, while its unique interactions with the opioid system suggest broader implications for the chronic pain crisis.
- This article summarizes the extensive data demonstrating DMSO’s efficacy for peripheral neurological conditions (approximately 600 studies and 400 pertinent reader testimonials), and concludes with practical guidance on DMSO protocols and the most potent DMSO pain formulation.
Over the last two years, I have compiled an extensive series of articles, which through citing thousands of studies, made the case that DMSO cures or improves a wide variety of conditions in every organ system of the body (all of which are indexed here)—including many diseases that are widely considered incurable (e.g., COPD or vision loss). Corroborating this, thousands of readers who were inspired to try DMSO have submitted almost unbelievable testimonials (which I’ve compiled here), and this series has now received millions of views.
DMSO, in turn, has a variety of properties that make it remarkably well-suited to healing the nervous system, resulting in thousands upon thousands of studies being published. I have therefore attempted to collect and compile all of them, but because so many exist, regardless of how much I condensed them, it was not possible to fit them all into a single article. As such, this is the third part of a four-part series, and critical context for this article can be found in the previously published pieces.
How DMSO Heals the Brain and Transforms Neurology

This is the longest and most detailed part of the series (encompassing 2,000 published studies and 200 reader reports).
How DMSO Heals the Spine and Reverses Paralysis

The Evidence DMSO Could Save Millions From Brain and Spinal Injury
In the near future, this article will be significantly revised to include the additional stroke and traumatic brain injury data I’ve collected over the last year (e.g., many readers have now reported DMSO saved them from strokes).
In turn, I have received many nearly unbelievable reports from readers, such as a mother rescuing her son from a life of paraplegia with DMSO (creating a story so miraculous that many news stations chronicled Jackson’s recovery from his hockey injury)
Likewise, another reader shared an equally extraordinary case (that Mary Beth Pfeiffer directly verified with the patient)

Finally, consider this case of terminal ALS (and brain fog) rapidly transforming into full functionality:
Note: we are now interviewing readers with remarkable DMSO stories they shared with us, but unfortunately lost the contact information for a few of the readers who used DMSO to treat the following conditions: colorblindness (becoming able to differentiate pink from orange or red), terminal pulmonary fibrosis, the son in the UK with fibrodysplasia ossificans progressiva, and sudden hearing loss in both ears that began in Taiwan. If you could contact me again, or email Dan (who is helping Rebecca compile testimonials) at [email protected] that would be greatly appreciated. Likewise, if you have a compelling DMSO story to share, please contact them at that address or leave a comment here—it will help a lot of people.
Nonetheless, all of this has provoked an understandable degree of skepticism—something being able to do this goes against many of the precepts modern medicine revolved around as it chooses to follow a biochemical model where change is created by affecting specific molecular targets rather (with a discrete number of effects), a choice I believe arose because this framework allows a nearly infinite number of patentable (narrowly focused) drugs to be made. In contrast, other marginalized models of medicine, such as the biophysical framework exist which provide a means for agents to affect a large number of diseases (and in many cases, unlike biochemical agents, address their root causes).
Because of this, I have tried to detail the evidence for every known mechanism of action of DMSO. Some of these include:
- Blocking pain transmission, relaxing muscles, and inhibiting acetylcholinesterase.1
- Acting as a highly potent anti-inflammatory and free radical scavenging agent.1,2
- Increasing circulation through histamine-induced vasodilation, stimulating lymphatic circulation, inhibiting numerous clotting pathways, and functioning as a targeted diuretic that eliminates harmful blood and fluid accumulation.1
- Stabilizing proteins (allowing them to regain lost function), neutralizing or dissolving damaged ones and scars, and preventing fibrosis.1,2
- Promoting microtubule polymerization and hence cell growth.1
- Neutralizing the smallest harmful microorganisms (which frequently trigger autoimmunity) by disrupting their membranes.1
These mechanisms partly explain the effects DMSO is repeatedly observed to create (e.g., its free radical scavenging and facilitation of DNA repair play a major role in protecting cells from otherwise lethal stressors like radiation, and its microcirculatory effects play a major role in its non-specific enhancement of immunity), while other therapeutic properties still lack any explanation (e.g., DMSO differentiating cells, including cancer cells, or reviving dying cells1,2).
However, once effects this broad are observed (affecting almost every part of the body), biophysical rather than biochemical means are typically needed to explain them, and I’ve hence tried to put forward those I believe best do so (e.g., to explain how DMSO produces remarkable results for a wide range of complex neurological and psychiatric illnesses I recently showed how DMSO directly separates blood cells by neutralizing the factors which cause them to clump together, thereby greatly increasing critical microcirculation throughout the body).
In this article, I will attempt to show how the same biophysical effects that produce DMSO’s two most well known effects—allowing substances to travel through cell membranes without damaging them and making cells able to survive being frozen—also underlie many of its other remarkable therapeutic properties and focus on their profound implications for the peripheral nervous system.
Cellular Resets:
When polar solvents (e.g., DMSO or water) are placed near a polar surface and provided with a radiant energy source (particularly infrared light), they will spontaneously form an aggregate that excludes particles or solutes from entering it, with water most effectively performing this transformation (becoming a gel-like liquid crystal). This was first observed by early biologists who saw this viscous liquid inside cells, and associating it with the fundamental substance of life, named it the “protoplasm,” then in the 1960s-1970s it was named “vicinal water” (because it formed in the vicinity of surfaces), after which it became known as interfacial water (a term that is routinely cited in the scientific literature).
Gerald Pollack, after concluding that water gels and their phase shifts to unstructured water were vital to physiology, realized this “liquid crystalline” state was a layered lattice of H3O2 surrounded by a layer of (displaced) H+ protons, and that in addition to it creating an “exclusion zone,” things could not pass through, was vital to physiology. Structurally, it effectively lubricated adjacent surfaces, protected linings (e.g., blood vessels) from damage, maintained the separation of suspended particles and served as the non-compressible units which provide the resilience and tensegrity (stability) of the body. Likewise, since this process creates a charge separation (H3O2– and H+) numerous energy gradients are created that biology can harvest (e.g., the charge separation creates a biological battery, and circulatory vessels both in animals and plants are structured so that the expelled protons, through mutual repulsion spontaneously drive fluid flow throughout the body). As such, a real case can be made that H3O2– is the perpetual motion machine which drives (and protects) biology because it will continually reform whenever it is broken down.
Note: I think about the above a lot due to its profound implications for biology—much of which I discuss here.
Gerald Pollack also believed it explained how nerves fired (action potentials) as:
•Biological systems use the gel-to-sol (H3O2– to H2O) phase transition to create energy and drive motion (after which H3O2– is restored). For example, when various anions were tested inside perfused axons, their ability to restore or destroy action potentials followed the Hofmeister series exactly: gel-stabilizing ions restored excitability (being ready to fire) while gel-solubilizing ions destroyed it.1
Note: every gel has a transition temperature where it will “melt” into a liquid. Since certain ions (e.g., calcium) can drop this temperature to below body temperature, the body’s targeted releases of Ca2 disperse the gels. Pollack originally argued this was due to calcium tightly binding together the biological polymers that gels otherwise formed around, but after discovering H3O2– switched to focusing on Ca2+’s Hofmeister effects (which I have also focused on too since the Hofmeister series strongly correlates with how ions affect zeta potential).
•A largely forgotten line of research by Tasaki1,2 and Matsumoto1,2 made the case that action potentials (nerve discharges) are not purely an ion channel event but a propagating phase transition in the peripheral cytoskeleton (the dense shell of actin and microtubules lining the inner membrane). The resting nerve maintains this gel in a compact, calcium-cross-linked state; stimulation triggers an abrupt swelling (as sodium displaces calcium and water rushes in), producing the electrical spike, after which the gel collapses back. In turn, dissolving the peripheral microtubules eliminated excitability; repolymerizing them restored it while stabilizing the cytoskeleton with DMSO or Taxol (at lower concentrations) enhanced excitability, indicating that nerve firing was directly linked to the phase of their cytoskeleton.
•The tendency of structured (liquid crystalline) H3O2– water to exclude solutes helps establish the cellular sodium-potassium balance. Structured water preferentially excludes sodium (because of its larger hydrated diameter) while better accommodating potassium. During the action potential, a phase transition causes the peripheral cytoskeletal gel to expand and hydrate. This breaks down the exclusion, allowing sodium to flood inward. As the gel later returns to its condensed state, potassium flows outward down its concentration gradient, completing the cycle.
•In one study, he showed that local and gas anesthetics (which pause nerve function) at minute concentrations enlarge the liquid crystal layer, whereas at higher (standard) concentrations they eliminate it, with bupivacaine being 4.5 times as effective as doing this as lidocaine (mirroring it being 4 times as potent an anesthetic as lidocaine).
Note: Pollack emphasized that the initial increase mirrors the excitation seen with general anesthesia prior to sedation, whereas I focused on the gel present, which reforms after the initial breakdown and is stabilized by residual lidocaine present.
Pollack’s observation and sensitive patients sharing that neural therapy injections seemed to unleash tiny rushes of fluid in their body (“it was as though a dam was opened”) eventually led me to postulate their actual mechanism of action was due to them dispersing pathologic accumulations of fluids within neurons (thereby restoring their normal firing thresholds) and outside cells (allowing blocked circulations, likely within the interstitial space) to resume. Furthermore, countless bodyworkers have observed that “trauma is stored within the fascia” (a structure that forms significant amounts of liquid crystalline water on the surface) and that releasing the fascia will cause emotional trauma to be released into the body—so I’ve come to wonder if pathologic configurations of liquid crystalline water can create both physical and psychiatric issues (particularly since neural therapy can sometimes profoundly change trauma patterns).
Note: One of the deepest unsolved problems in science is the origin of subjective consciousness — the “hard problem.” A controversial but increasingly considered theory proposes that quantum computations inside neuronal microtubules (which are directly affected by the cell’s gel-like phase) play a key role in generating conscious moments. The model notes that healthy neurons contain specialized microtubule-associated proteins that stabilize these polymers, potentially allowing the coherence required for such quantum processes.
Given all of this, it immediately caught my eye that many of the DMSO studies I saw noted it stabilized microtubules, actin filaments, and cell membranes, particularly since the effects are reversible and DMSO (due to its permeability) rapidly washes out of cells, ensuring the change amounts to a temporary “reset” of cellular structure that could potentially restore cells to a healthy organized state. Likewise, I spent a while trying to understand how these stabilizing effects could occur concurrently with DMSO also temporarily fluidizing the membrane and increasing cell permeability, since these descriptions appear contradictory. However, they are actually complementary, reflecting concentration-dependent actions of the same molecule on the same structure.
How DMSO Affects Cellular Structure
Note: this section is a bit technical, and not critical to understand if you’ve read the preceding paragraph so you may want to skim it. I am including it mostly because I spent a long time trying to figure this out and I know a subset of readers will be very interested in it too.
At the molecular level, DMSO forms strong hydrogen bonds with water (the DMSO-water interaction is stronger than water-water bonding1), and at 37-45%, DMSO creates chain-like molecular associations with water that enhance local hydrophobicity,1 while at higher concentrations it can induce liquid-liquid phase separation in water itself, producing regions with structurally distinct water configurations.1 Likewise, DMSO is inherently viscous (thick) and increases the viscosity of water by structuring it,1,2,3 which can be seen when the two mix together (and is why DMSO will exothermically create heat when it mixes with water).
When DMSO is poured into water, the two liquids do not simply mix. Instead, as this video shows, the combination produces slow, viscous, gel-like flows with persistent boundaries and transient ordered regions that bear a remarkable resemblance to the “protoplasm” early biologists observed inside living cells (we hence found ourselves unable to stop watching, eventually adding a dye to make the structured phases easier to see). That said, I’m still not sure if this macroscopic phenomenon is a direct representation of the microscopic clustering that occurs when DMSO mixes with water, but regardless, it provides an excellent visual metaphor to understand what will be described in the sections that follow.
Opening or Solidifying the Cell Membrane
One of DMSO’s most unique properties is that it passes through biological membranes without damaging them (including the blood-brain barrier)1,2,3 and temporarily increases the permeability of organic membranes to other substances. This appears to result from how DMSO shifts the water within the cell membrane (which then reverts once DMSO readily diffuses away).
At low-to-moderate concentrations (roughly 1–10%), DMSO acts as a kosmotrope (a water-structuring agent) that dehydrates phospholipid headgroups by displacing approximately 45% of the surface water layer, compresses inter-bilayer water layers,1,2,3,4,5 raises phase-transition temperatures,1,2,3,4,5,6,7 and stabilizes tightly packed gel phases at the expense of looser fluid phases.1,2 Finally, at higher concentrations (e.g., 44%), this dehydration becomes complete, with neighboring DPPC bilayers fully pressed together and no intermembrane water layer remaining.1
X-ray diffraction studies showed that this compression is not driven by DMSO penetrating into the membrane, but rather by DMSO forming clusters with water molecules at the membrane surface. Because DMSO interacts more strongly with bulk water than with the membrane, these clusters osmotically pull water away from the lipids, compressing the membrane and forcing the lipid chains to pack more tightly and stand more vertically.1,2,3,4 Corroborating this, DMSO reduced water permeability across mammalian cell membranes by about half,1 and at the picosecond scale, low concentrations slowed lipid motions while creating a more dynamically ordered bilayer at the lipid-water interface.1
Overhauser dynamic nuclear polarization also confirmed this surface-level action: below 30%, DMSO exclusively weakened the water network at the membrane interface without altering bilayer thickness or headgroup mobility,1 decreasing the repulsive forces between bilayers (allowing them to approach much more closely).1,2 Furthermore, since each DMSO molecule was similar in size to a membrane lipid headgroup (480 ų), low DMSO concentrations could effectively compete for headgroup hydration water (and dehydrate the membrane).1
In short, the overall membrane bilayer remains intact, its basic architecture is protected against stress, and the membrane becomes noticeably less permeable. Numerous studies support this picture,1,2,3,4,5,6,7,8,9 and the same stabilizing effect has been consistently observed across the major components of cell membranes — including phosphatidylcholines,1,2 phosphatidylethanolamines,1,2,3,4 sphingomyelins,1,2 and mixed lipid systems that more closely resemble real cell membranes.1,2
Note: this stabilizing effect has also been shown to reduce the ability of pathogens like Toxoplasma to penetrate and infect cells.
At somewhat higher local concentrations, the picture shifts.1,2,3,4,5,6 Studies on cholesterol-containing membranes and live cells have identified three distinct stages. At 10% or below, DMSO inserts into the headgroup region, thins the bilayer, spreads lipid molecules farther apart, and loosens their fatty tails, creating visible ripples but no stable pores. Between 15–20%, stable water-filled pores form (structural defects spanning the full thickness of the bilayer), allowing ions to enter and causing cell swelling. Above 20–30%, multiple pores appear, the membrane develops extreme undulations, and eventually (at higher concentrations than can be sustained with medical DMSO applications) begins to break apart.1,2,3 Atomic-scale simulations confirmed the same three stages.1,2,3
These pores have been confirmed in live cells at concentrations as low as 0.1% (using fluorescence imaging of thallium and calcium influx), with visible membrane blebbing appearing at 2%. The pores are non-selective — both positive and negative ions can pass through freely — and they are not blocked by conventional ion channel inhibitors, showing they are physical gaps in the lipid bilayer itself rather than normal protein channels.1
Lastly, DMSO was also found to shift the stereoisomeric conformation of membrane fatty acids from cis to trans forms, potentially creating micropores through a mechanism distinct from the pore-formation pathway described above.1
Note: DMSO’s permeabilizing effect also extends to intracellular membranes. For example, DMSO (5–25%) progressively increased lysosomal membrane permeability in a concentration-dependent manner (allowing sequestered enzymes to access and eliminate degenerative cellular waste products)—providing another mechanism for how DMSO treats neurodegenerative disorders.
These temporary dose-dependent biphasic effects are also seen in a variety of lipids and (phospholipid) cellular membranes:
•In ceramides (the predominant lipid in the outermost layer of the skin), below roughly 60%, DMSO accumulated at the ceramide-water interface, displacing water and forming hydrogen bonds with ceramide headgroups while leaving the gel-phase bilayer structure intact. Above roughly 70%, DMSO integration into the headgroup region replaced ceramide-ceramide hydrogen bonds (reducing them from 2.8 to approximately 1.1 per molecule), destroying the lateral hydrogen-bonding network that gives skin its barrier rigidity and triggering a complete phase transition from an ordered gel phase to a permeable liquid-crystalline phase.1,2,3,4,5
•In muscles, DMSO at 5–10% induced extensive true membrane fusion in sarcoplasmic reticulum vesicles (individual vesicles flattened, established contact, and merged into continuous bilayer sheets), while 25% paradoxically prevented fusion by inducing initial rigidity, and overnight exposure at 10–25% destroyed fused structures entirely, revealing a narrow structural window for productive fusion.1,2
•In phospholipid vesicles, electron microscopy showed DMSO promoted whole-membrane fusion (as opposed to simple lipid exchange).1,2 This fusion-modulating effect extends to neurotransmitter release: at the single-vesicle level, 0.6% DMSO increased the fraction of catecholamine released per exocytotic event from approximately 53% to 92% and accelerated release kinetics1—likely by causing pores to open more fully or remain open longer, providing an additional mechanism by which DMSO treats neurological disorders (such as myasthenia gravis).
•In human red blood cells, DMSO protects against hypotonic hemolysis by increasing the critical volume the cells can swell to before bursting, with this protective effect increasing with DMSO concentration up to 23–25% (beyond which hemolysis occurs instead).1 In a separate study on membrane mechanics, 1% DMSO increased the RBC bending modulus (stiffening) by approximately 37%, 5% DMSO softened it, and 10% DMSO produced only weak, transient effects.1
Note: the authors of one of those studies highlighted that DMSO’s membrane actions resembled those of anesthetics—an observation corroborated by fifty years of subsequent research (and potentially another way in which DMSO reduces pain).1
•In intestinal cells DMSO initially raised polarization (decreased fluidity) but then induced a transient fluid phase before returning to baseline, a temporal sequence consistent with the reset model.1
•In yeast cells, approximately 10% DMSO enhanced DNA transformation efficiency 25-fold by transiently permeabilizing the plasma membrane without reducing cell viability.1,2
This permeability-enhancing effect is not universal at low concentrations, however: in barnacle cells very low concentrations did not change membrane permeability,1 while in E. Coli membranes, 7.8% DMSO reduced rather than increased permeability.1
Lastly, the specific structural effects DMSO produces on membranes depend on lipid composition (and phase as DMSO preferentially interacts with membranes in the fluid phase). Membranes made from unsaturated lipids (DOPC) are significantly more resistant to DMSO’s structural disruption than those from saturated lipids (DPPC),1 and negatively charged headgroups (DMPG) are less affected than zwitterionic ones (DMPC, DPPC), suggesting DMSO preferentially interacts with the positively charged choline moiety.1 These compositional dependencies mean DMSO’s effects in living tissues will be heterogeneous and cell-type-specific1,2 (as the above examples show), which may contribute to its selective normalization of pathological states rather than uniform disruption.
Note: individuals who adopt seed oil free diets (e.g., carnivore) frequently report improved skin tolerance to sun, indicating that a membrane change has occurred. Likewise, some DMSO users report that once they clean up their diet and detoxify their bodies, their DMSO odor (which only affects a portion of users) improves. This suggests that diet-induced lipid changes can either make DMSO more effective or reduce its odor: greater membrane permeability would help DMSO reach hepatocyte microsomes, where it is oxidized to the odorless DMSO2, whereas a higher PUFA intake would work against this and furthermore would promote inflammatory gut dysbiosis and a rise in species that reduce DMSO to the odor-producing DMS. Other approaches for reducing DMSO’s odor are discussed here.
Resetting the Cytoskeleton
By temporarily shifting cell membranes into a more fluid (sol) state, DMSO enables them to reorganize and reform in a healthier configuration. For example, in pure water at room temperature, DHPC membranes form an atypical interdigitated gel phase (where the fatty tails from opposing membrane layers poke into each other). DMSO (12%) reversed this non-physiological state to the normal bilayer gel phase while stabilizing it by raising its melting temperature — actively favoring the physiologic configuration that supports normal membrane function.
In the case of the cytoskeleton (which primarily shapes the entire cell), while DMSO consistently stabilizes key structural components — microtubules along with the vimentin-based intermediate filament network (preventing its breakdown under cyclic hydrostatic pressure1) — it readily diffuses after creating that stabilization, also providing a reversible, cyclic reset for actin, the most abundant cytoskeletal protein (which is responsible for cell shape, motility, adhesion, and mechanical tension).
In a series of studies spanning slime molds, human HeLa cells, rat fibroblasts, kidney cells, and cultured hippocampal neurons, DMSO (typically at 5–10%) was shown to rapidly dissolve cytoplasmic actin stress fibers and simultaneously drive the released actin into the nucleus, where it reorganized into massive, ordered filamentous bundles.1,2,3, 4,5,6,7,8,9,10,11,12,13
These reversible changes are also tightly controlled. Nuclear actin bundles appear within 20–30 minutes of DMSO exposure, and upon DMSO removal (as DMSO freely diffuses out of cells), they disappear within 5 minutes, with complete restoration of cytoplasmic stress fibers and normal cell shape within 1–2 hours.1,2 The effect requires concentrations of at least 3% (below which no cytoskeletal changes occur1), is optimal at 5–10%, and becomes irreversible above 20% (where cells appear fixed and disorganized with no paracrystal formation).1 Fluorescent skeletal muscle myosin light chains incorporated into live nonmuscle stress fibers also showed the same dynamic reset: DMSO dispersed them into the cytoplasm, and removal triggered their reformation within 45 min.1
Note: the last study provides an alternative mechanism to explain how DMSO relaxes muscles, particularly persistent contractures.
Furthermore:
•Fluorescent actin microinjection directly proved the translocation pathway: labeled actin incorporated into stress fibers, then upon DMSO addition the fluorescent fibers dissolved and fluorescent inclusions appeared in the nucleus, with complete reversal on washout.1
•This translocation is molecularly specific. Tropomyosin, alpha-actinin, and myosin (the other major stress fiber components) remain in the cytoplasm,1,2 while actin translocates to the nucleus (along with cofilin and actin depolymerizing factor—which co-localize with actin to form intranuclear rods).1,2,3,4
•This effect is seen in a wide range of species (e.g., amoebae, slime molds, Tetrahymena, rat kangaroo cells and human cells1,2,3,4)indicating DMSO acts on a fundamental property of actin itself rather than a specific molecular target. Likewise, the process does not require new protein synthesis or energy to maintain (bundles persist even under ATP depletion)—though initial formation does require ATP—pointing to a direct physicochemical action of DMSO on actin rather than a gene-expression-mediated process.1,2
DMSO’s temporary remodeling also caused a variety of other similar changes in cytoskeletons:
• In rat embryo fibroblasts, 3–10% DMSO rapidly disrupted organized actin cables into a diffuse distribution and caused cell retraction (73% of cells at 10% DMSO within 15 min). Upon washout, 91–97% of cells fully respread and reformed actin cables within one hour.1
•In hepatocytes, 2% DMSO (plus trace glucagon) rapidly converted flat, spread cells into compact cuboidal forms, reorganizing F-actin into perijunctional rings and triggering a sharp rise in cytosolic calcium.1 DMSO also shifted primary hepatocytes from flattened to polygonal/spherical shapes, depolymerizing dense intracellular F-actin and repolymerizing it into a submembranous cortical layer, while dispersing vinculin from focal adhesions and redistributing fibronectin to cell-cell contacts (enabling long-term culture exceeding one month),1 while DMSO alone induced elaborate polygonal actin networks (“geodomes”) without altering total actin levels, indicating post-translational reorganization.1
•In kidney mesangial cells, 10% DMSO caused rapid, reversible loss of contractility (disappearance of surface wrinkles within 10 minutes, reappearing upon washout).1
In addition to facilitating a “cellular reset,” other direct benefits resulted from this process:
•DMSO disassembled stress fibers and caused transient cytoplasmic relocation of talin (which anchors actin stress fibers to focal adhesions) away from adhesion sites; upon washout, talin returned to its normal position and actin cables fully reformed (potentially providing a mechanism to explain the benefits seen from using DMSO to treat problematic adhesions).1
• In neurons, DMSO triggered rapid translocation of actin and actin-polymerizing factors from growth cones into the nucleus, temporarily halting neurite outgrowth. Upon removal, these components returned to the growth cones, and motility was fully restored — demonstrating a reversible “disarm and re-arm” of the axonal growth machinery with potential relevance for resetting nerve regeneration.1,2,3
•In growth cone membranes, high DMSO concentrations reduced bending modulus and surface tension, lowering effective viscosity by promoting slip between the membrane and cytoskeleton (the dominant resistance to deformation) and thereby facilitating protrusion formation for axonal extension.1 Low concentrations of DMSO also disrupted the axonal initial segment diffusion barrier, allowing redistribution of polarized membrane proteins.1 Supporting this, 2% DMSO dramatically increased membrane tether length in human mesenchymal stem cells and fibroblasts (comparable to combined cytoskeleton disruption and cholesterol depletion), confirming that DMSO temporarily weakens membrane-cytoskeleton coupling and enhances membrane reservoir availability.1
•Tissue repair typically begins with the formation of a provisional gel-like matrix (composed of hyaluronan, fibrin, collagen, and structured water) that serves as the scaffold for cell migration and proliferation. As DMSO stabilizes numerous gel states,1 (along with switching biomolecules like urea from opposing to supporting gel formation1) this provides another mechanism to explain DMSO’s ability to facilitate tissue healing.
Note: similarly, DMSO enhances plant healing. In one potato study, accelerated wound healing of potatoes by thickening their protective suberin layer and forming a stronger cork-like wound-sealing barrier on cut surfaces.
Another one of DMSO’s unique properties is that it will cause a wide range of cancer cells to differentiate (revert to normal); however exactly why it does this remains unknown. Since numerous polar solvents besides DMSO have also been observed to trigger differentiation,1,2,3,4 (and form liquid crystalline aggregates) and studies have shown the state of the cytoplasm mediates malignancy1,2,3,4 (e.g., cytoplasms from cancerous cells are highly carcinogenic whereas cytoplasms from normal cells reduces cancer cell growth and can drive differentiation), I was curious if physical changes from DMSO (e.g., it reorganizing the disordered cytoplasm frequently found in cancer cells) could be driving this effect. Studies, in turn, show:
•When Friend erythroleukemia cells are differentiated by DMSO membrane, fluorescence polarization increased, capacitance dropped by approximately 30% and conductivity decreases more than 5-fold, indicating that the membrane became physically tighter and less conductive as cells matured from a cancerous to a more normal phenotype.1,2 Additionally, actin progressively shifted from its soluble (G-actin) form toward its filamentous (F-actin) form, with the G/F-actin ratio decreasing steadily as cells matured, reflecting cytoskeletal stabilization.1
•In HL-60 leukemia cells, DMSO-induced differentiation normalized F-actin content in non-dividing cells to levels matching non-cancerous cells, an effect that did not occur in non-differentiable cell lines.1 DMSO also increased total actin 1.8-fold and drove gelsolin-mediated filament shortening that restructured the cytoskeleton to parallel normal neutrophils.1 The maturation also enabled entirely new cytoskeletal responses: non-differentiated HL-60 cells showed no F-actin increase when stimulated, while DMSO-differentiated cells acquired rapid 30–50% F-actin increases and pseudopod formation, reflecting acquisition of mature actin regulatory mechanisms.1
•A 2022 study showed these cytoskeletal effects are highly cell-type specific. In normal skin cells, 1% DMSO strengthened the cytoskeleton by increasing F-actin and repositioning vinculin for better structural anchoring. In melanoma cells, it weakened pathological architecture and cancer invasiveness by reducing vinculin and shifting F-actin from rigid linear bundles to a more branched form. Adding calcium sulfide amplified this disruptive effect on cancer cells while leaving normal cells unaffected.
Lastly, DMSO’s best known use is for cryopreservation, which it accomplishes by vitrifying the cells, so that when they freeze, rather than ice crystals forming (which destroy cells), they become a disordered vitreous (glass-like) amorphous solid due to the same headgroup dehydration, gel-phase stabilization, and controlled membrane-fluidity modulation described above1,2—all of which fully reverses once the cell thaws—again demonstrating that DMSO can guide cells through phase transitions without damaging cells.
Note: the concentrations at which DMSO raised phospholipid phase transition temperatures (stabilizing membrane gel phases) correlated directly with the concentrations at which it induced differentiation of Friend leukemia cells. This correlation also held for other cryoprotective agents and divalent cations (which similarly raised transition temperatures), as well as for local anesthetics (which produced opposing effects by lowering the phase transition temperature and inhibiting differentiation).1,2,3,4,5—all of which suggests DMSO’s membrane-stabilizing actions and its differentiation-inducing properties share a common structural mechanism.
Lastly, when used to treat chronic pain, it is frequently observed the best results are obtained with periodic breaks and several readers here independently discovered this. One with a complex neck/shoulder injury observed: “It seems that I would get the best response if I use an ON-OFF strategy: Apply DMSO for several days then stop for a day or two… when I stopped with DMSO, the pain would at first increase then over the course of the following day reach a new low. It’s almost as if DMSO attenuates some useful signals to the body, which after its removal is able to better ‘see’ where the problems really are and heal.”1 The Parkinson’s researcher similarly found “I always feel my best the day after I stop DMSO” and explored pulsed dosing.1 This pattern is consistent with the cellular reset model described earlier in this article, where DMSO’s temporary structural reorganization may need to be followed by a consolidation period for the body to establish a new baseline.
Peripheral Nerve Regeneration & Protection
One of DMSO’s most remarkable properties is its ability to facilitate regeneration of the central nervous system (which otherwise does not heal), due to its having a variety of properties including:
- Powerfully facilitating the polymerization of microtubules—which cells require to divide (discussed in the first article)
- Differentiating stem cells into neurons (both of which were discussed in the previous article)
- Restoring circulation to the nerves (discussed in the first article)
- Stabilizing cell membranes (discussed above) and reducing chronic inflammation (which often disrupts cellular repair)
- Preventing demyelination and promoting remyelination (discussed below and in the first article).
- Enhancing electric field-induced nerve branching (new branch growth from existing nerves is how damaged neural pathways reconnect, a process the CNS environment normally suppresses).
Peripheral nerves, unlike those in the brain and spinal cord, possess an innate capacity to regenerate after injury. However, this process is slow (approximately 1 mm per day), frequently incomplete, and often complicated by scarring, inflammation, and loss of the supporting Schwann cells that myelinate nerves (with surgical approaches such as direct repair or autologous nerve grafting being the gold standard, but producing inconsistent results, particularly for severe injuries with gaps or delayed treatment). Fortunately, DMSO’s ability to heal the central nervous system also translates to it regenerating peripheral nerve injuries.
DMSO-Alone Findings
Several studies have directly demonstrated that DMSO promotes peripheral nerve regeneration and that local DMSO application consistently outperformed systemic (intraperitoneal) administration:1,2,3
•In rats whose sciatic nerve was transected, local or intraperitoneal DMSO improved regeneration and reduced perineural adhesions, with significant gains over untreated controls across multiple metrics: gastrocnemius muscle weight ratio (+50%), nerve growth factor expression (+227%), myelin basic protein expression (+165%), myelinated axon counts (+26%), compound motor action potential amplitude (+935%), conduction velocity (+303%), and toe-spread test scores (+50%).1,2
•In a neurotmesis model (severing the nerve and each of its protective sheaths), 10% DMSO applied locally at the repair site for 12 weeks acted as an antioxidant, anti-inflammatory, and antifibrotic agent, significantly improving nerve healing: higher gastrocnemius muscle weight ratios, better macroscopic nerve scores with reduced adhesions, increased NGF and MBP (nerve-repair proteins) expression, thicker myelin sheaths, larger axon diameters, higher myelinated axon counts, improved nerve conduction (higher CMAP amplitude and conduction velocity), and better functional outcomes on pinprick and toe-spread (sensory and motor) tests.
•In rabbits with sciatic nerve compression, topical 50% DMSO promoted nerve regeneration as confirmed by functional testing, electromyography, and histopathology,1,2 (corroborating DMSO’s efficacy in treating compression neuropathies).
•DMSO also promoted Schwann cell proliferation after nerve injury: in a sciatic nerve crush model, the vehicle control group receiving 10% DMSO showed significantly higher Ki67-positive Schwann cell expression.
•When DMSO was used as the fill agent within eggshell membrane nerve guidance channels bridging 1 cm rat sciatic nerve defects, it produced superior outcomes to autograft in several measures: higher Sciatic Functional Index scores (assessed by walking), greater myelinated axon counts, and significantly better muscle weight preservation at 90 days.
DMSO also directly protects nerves from injury:
•In cultured rat superior cervical ganglia, local application of DMSO delayed axon degeneration for up to 12 hours by preserving axonal structure and slowing microtubule degradation, with a protective effect comparable to overexpression of the WldS protein (a well-established standard for preventing axonal degeneration in nerve protection research).1,2
•In frog and rabbit sciatic nerves, DMSO protected them from freezing damage1,2,3,4
•0.00078% DMSO preserved bioelectrical activity in a group of nerve fibers exposed to UV radiation.
Note: in the first part of this series, I showed that DMSO protects cells and organs throughout the body (particularly in the brain and spinal cord) from a wide range of otherwise lethal stressors.
Numerous readers have reported that DMSO regenerated and repaired their nerves. Two of the most remarkable ones were:
•A reader’s husband developed drop foot from a fall compressing a nerve, with the front leg muscles “basically dying” and pain severe enough to require near-overdose levels of opioids. DMSO was “a massive game changer, the only thing giving relief from nerve damage.” After eight weeks of topical use, “muscle had started growing back, an inch above ankle and inch below knee, which Neurosurgeon has no answer for and is in disbelief.” This muscle regrowth enabled a compression test and subsequent nerve release surgery, and two weeks post-surgery, he was walking better without his foot brace.1
•Rebecca (who has been filming the DMSO testimonials I’ve posted like Todd’s) had her lower leg crushed in an accident over 10 years ago, requiring multiple surgeries, tissue transfer, and skin grafts. Despite numerous treatments, she had persistent poor circulation and extensive numbness throughout the scarred area. After two weeks of daily DMSO with aloe vera,⬖ blood flow visibly increased into tissue that had turned gray and purple, sensation began returning to areas numb for 9.5 years, and as time goes on, more sensation returns.¹
Axolemmal Resealing
When nerve fibers are cut or crushed, the ruptured membrane must reseal rapidly to prevent cell death. DMSO has been shown to significantly enhance this critical repair step. In guinea pig spinal cord white matter, 5% DMSO enhanced axolemmal resealing under conditions of low calcium or low temperature (improving membrane potential recovery by approximately 21-23% and markedly reducing unrepaired axons), conditions that otherwise severely impair the repair process.
Similarly, in rat dorsal root axons in vivo, 0.5-5% DMSO significantly enhanced resealing in low-calcium conditions to levels comparable to normal physiological calcium, likely by disrupting the submembranous actin network and facilitating membrane reorganization.
Even at very low concentrations (0.00064-0.2%), DMSO significantly increased axolemmal sealing frequencies in hippocampal-derived neuroblastoma cells, likely by enhancing Ca²⁺ influx and vesicle fusion.
Limb Regeneration
DMSO’s regenerative potential extends beyond nerve repair to whole-limb regeneration. In postmetamorphic bullfrogs (which normally cannot regenerate amputated limbs), repeated topical DMSO immersions of the amputated stump induced substantial regeneration in 100% of cases by 120 days, containing multiple cartilage elements, striated muscle, and evidence of bone remodeling.1
DMSO appeared to promote cellular dedifferentiation and blastema formation, effectively unlocking latent regenerative capacity in these normally non-regenerating animals. In adult newts, a single systemic exposure to DMSO accelerated limb regeneration by approximately 48-72 hours, with markedly higher lysosomal hydrolase activity during the critical early phase, supporting enhanced tissue reorganization.1,2
Neuronal Differentiation
As I showed in the previous article, a large number of studies show DMSO induces neural differentiation, thereby providing a way for the body’s stem cells to repair damaged nervous tissue.
In one particularly relevant study of N1E-115 neuroblastoma cells, 1.5% DMSO for 48 hours reproducibly triggered neuronal characteristics (neurite outgrowth, functional excitability) without elevating intracellular calcium or triggering cell death.1,2 When these DMSO-differentiated cells were seeded onto biomaterial scaffolds and implanted at peripheral nerve injury sites, they remained viable and continued to secrete neurotrophic factors at near-physiological concentrations at the implantation site for the entire regeneration periods studied (12 weeks for axonotmesis and 20 weeks for neurotmesis), creating a supportive local microenvironment for axonal regrowth, Schwann cell migration, and remyelination.1 The differentiated cells maintained viability on chitosan membranes and other biomaterial scaffolds, supporting their potential for peripheral nerve tissue engineering.1,2 Finally, when PLGA 90:10 tube-guides (with or without DMSO-differentiated cells) were used to bridge 10 mm rat sciatic nerve gaps, significant motor and sensory functional recovery was achieved in both groups over 20 weeks (comparable to each other, though inferior to autologous graft).1
Dose-Dependent Regeneration
DMSO’s effects on nerve conduction are concentration-dependent and biphasic. At very low concentrations (0.01–0.1%), no effects on axonal transport,1 action potential propagation,1 or fast axonal transport1 have been detected. At low concentrations (≤1%), DMSO enhances synaptic transmission and promotes neuronal repair.
In mollusk neurons, concentrations up to 0.8% produced no significant changes in resting potential or ionic currents, while 4-8% caused reversible depolarization with altered firing patterns.1,2
At higher concentrations (5–10%), it can reversibly disrupt fast axonal transport1,2,3 and slow nerve conduction velocity or block it1,2,3,4 (which likely contributes to its analgesic [pain reducing] properties). At the highest concentrations studied systemically (7.8% intraperitoneally for 10 days in rats—a concentration far exceeding what standard DMSO dosing can reach), reversible structural changes to myelin were observed (uncompacted lamellae, axonal swelling) with full functional recovery by day 55, while no structural changes occurred at 1.8% or 3.6%.1 Likewise, when concentrated DMSO (33% or 100%) was injected perineurally around the rat sciatic nerve, dose-dependent (but recoverable) nerve injuries occurred.1,2
This helps to explain why while DMSO typically aids nerve regeneration one early study found topical 90% DMSO applied under the skin directly to a nerve repair site (resulting in much higher concentrations than 90% DMSO applied to the skin above a nerve) had no measurable effect on regeneration rate or quality (though treated animals had fewer auto-amputated toes and finer scar lines).1
Note: intraperitoneal DMSO (which creates higher DMSO levels than topical applications) had no adverse impact on olfactory neuroepithelium, axon pathways, regeneration, or targeting, confirming the safety of systemic applications for nerves.1
Synaptic Transmission and Neuromuscular Function
DMSO directly enhances neurotransmitter release at synapses and neuromuscular junctions:
•In frog neuromuscular preparations, DMSO (0.5-5%) acted as a fusogenic agent that promoted synaptic vesicle fusion with the nerve terminal membrane, markedly elevating spontaneous acetylcholine release even in near-calcium-free conditions and increasing evoked release 2- to 19-fold depending on concentration and calcium levels.
•In guinea pig tracheal spirals, 1% DMSO caused a 13% increase in electrically induced muscle contractions.
•In bullfrog sympathetic ganglia, DMSO (3-10%) restored synaptic transmission under low-calcium conditions that would otherwise impair signaling, preserving acetylcholine release and even inducing repetitive firing from a single stimulus.
•In frog sympathetic ganglia, DMSO enhanced synaptic transmission by increasing and prolonging fast excitatory postsynaptic potentials, likely through interference with potassium permeability.
•DMSO potentiated synaptic transmission at the rat superior cervical ganglion prior to neostigmine treatment.
Note: in garter snakes, 0.5% DMSO had no effect on spontaneous acetylcholine release or resting membrane potential, but did increase endplate current amplitudes and prolong their time courses, consistent with its known acetylcholinesterase inhibiting activity. Likewise, at the squid synapse, neither DMSO (0.1%) nor nitrendipine affected transmission.
Additionally, DMSO has a particular affinity for adrenergic (sympathetic) nerve tissue: when added to glyoxylic acid histochemical preparations, DMSO markedly improved the visualization of adrenergic nerve elements, consistent with enhanced penetration and concentration within these structures.
Combination Studies in Peripheral Nerve Models
In many studies and patents, DMSO is used to deliver (and potentiate) an agent, where in many cases, the therapeutic properties of the combination resemble what DMSO alone does (and in some cases, the study makes it possible to independently assess the effects of DMSO, where often, a benefit from DMSO alone is observed—but often not mentioned in the article’s summary). In this series, I have included the combination studies for you to skim through both because they shed light on possible therapeutic effects of DMSO (particularly if common benefits are seen across multiple combinations) and because they provide ideas for therapeutic combinations readers can utilize (with natural agents that were combined with DMSO being marked with a ⬖ to support readers exploring combination options).
Note: I believe a key reason lab results are frequently not seen in humans is because lab studies often use DMSO whereas human studies only use the agent.
For example, DMSO (in 5–50% aqueous solutions) has been repeatedly described in the Russian literature as a universal solvent for topical iontophoretic (electrical) delivery in peripheral nervous system diseases (including neuritis and neuralgia of the facial, radial, ulnar, femoral, sciatic, and tibial nerves), as it enhances drug penetration and pharmacological activity and enables iontophoretic treatment with water-insoluble medications.1,2
Numerous DMSO combinations have hence been used to treat nerve injuries. These include:
•Histamine transiently improved pain and touch perception at leprosy lesions in 31–47% of patients (depending on concentration).1
•A peripheral nerve injury patent using DMSO mixed with spasmolytic medications applied over specific anatomical zones under a pulsating magnetic field.1
•Another patent that used topical stephaglabrine sulfate⬖ in a DMSO-containing base.1
Likewise, a large number of agents dissolved in DMSO have demonstrated therapeutic benefit in peripheral nerve injury models (following sciatic nerve injury):
•Curcumin⬖ promoted Schwann cell autophagy, reduced apoptosis, and facilitated myelination and axon regeneration through the Erk1/2 and Akt pathway.1
•Resveratrol⬖ improved motor function and upregulated NeuN/MAP2 with preserved anterior horn neuron numbers.1
•Rapamycin enhanced autophagy, increased LC3-II expression, promoted motor recovery (2-fold higher stand time at 1-2 weeks), increased myelin basic protein and neurofilament-200 immunoreactivity, and reduced Schwann cell apoptosis.1
•Pterostilbene⬖ further increased Schwann cell proliferation beyond DMSO alone, improved sciatic nerve function, upregulated autophagy markers, and increased myelin thickness.1
•Lycopene⬖ (in eggshell membrane nerve guidance channels) achieved superior functional recovery, muscle preservation, myelinated axon counts, myelin thickness, and Schwann cell density comparable to autograft.1,2
•Minocycline attenuated the neuroinflammatory cascade that perpetuates nerve injury, suppressed spinal microglial activation, reduced BDNF upregulation, and inhibited PI3K and ERK phosphorylation (with comparable efficacy to local pulsed radiofrequency).1,2
Among agents targeting specific pathways, a ROCK inhibitor enhanced axonal regeneration, growth cone expansion, Schwann cell proliferation, remyelination, and functional recovery via PI3K/GSK3β signaling, a caspase-1 inhibitor reduced Schwann cell pyroptosis, demyelination, and reactive oxygen species through Nrf2/HO-1 modulation, an HDAC6 inhibitor (Tubastatin A) reduced dorsal root ganglion neuronal apoptosis and improved sensory function in a cauda equina compression model and a p38MAPK inhibitor ameliorated skeletal muscle fibrosis and reduced connective tissue growth factor expression after chronic nerve compression.
Additional agents showing neuroprotective or pro-regenerative effects for peripheral nerves include an FK506 inducer (promoted Schwann cell differentiation with increased GFAP and NF200 expression), clobetasol (enhanced Schwann cell proliferation and NRG1/EGR2 expression in sericin nerve conduits, achieving recovery comparable to autograft), chondroitinase ABC combined with intracellular sigma peptide (promoted axon regeneration and motor neuron survival in brachial plexus avulsion), and tetramethylpyrazine⬖ (induced bone marrow mesenchymal stem cell neural differentiation, significantly improving motor function, evoked potentials, and NGF expression after sciatic nerve injury).
Among agents promoting axonal outgrowth across inhibitory barriers, diltiazem enhanced axon regeneration up to 2-fold in adult mouse DRG neurons on inhibitory CSPG substrates and similarly promoted outgrowth in human induced sensory neurons, while quercetin⬖ and genistein⬖ enhanced NGF-induced neurite outgrowth in PC12 cells via Na⁺/K⁺/2Cl⁻ cotransporter activation and nimodipine (which enhanced NGF-induced neurite outgrowth from neurons in a concentration-dependent manner while protecting against ethanol and osmotic stress-induced cytotoxicity). Miconazole reversed organophosphate-induced delayed neuropathy in hens, restoring Nissl bodies, sciatic nerve S100β, and myelin basic protein expression while normalizing ErbB3/Akt signaling.
DMSO combinations also counteracted the neuropsychiatric consequences of nerve injuries. In rats, intrathecal (delivered into the CSF) rapamycin attenuated depression (triggered by spinal nerve ligation-induced neuropathic pain), increasing mechanical withdrawal thresholds, reducing forced swim immobility, and restoring prefrontal cortex autophagy (upregulating LC3 II/Beclin-1, downregulating p62). Likewise in rats, an α5-GABAAR inverse agonist reversed GABAergic cognitive impairment (lost recognition memory and spatial alternation) following sciatic nerve injury.
Note: the one drug which caused significant issues in combination with DMSO was sulindac (a now restricted NSAID) which sometimes caused neurotoxic reactions (e.g., there was one case of a profound mixed sensorimotor peripheral neuropathy 1,2,3,4) despite DMSO reducing sulindac’s bioactivity,1
Veterinary Applications
DMSO is used in veterinary practice for a variety of peripheral nerve conditions and has been cited in multiple veterinary textbooks and reviews as a conventional treatment for peripheral nerve conditions in dogs and horses (that is valued for its anti-inflammatory, analgesic, antioxidant, and tissue-penetrating properties). 1,2
In horses, published cases show IV DMSO contributed to recovery from temporohyoid osteoarthropathy with facial nerve and vestibular deficits,1 femoral nerve paralysis secondary to rhabdomyolysis (complete resolution by day 19),1 and post-anesthetic femoral neuropathy (one of two horses achieved full recovery after 6 months).1
Additionally:
•Topical DMSO applied as cold packs resolved bilateral radial nerve paralysis in a newborn foal with dystocia-related (birth trauma) compression injury.
•A rectal DMSO protocol (combined with an anti-inflammatory, vitamin E,⬖ and an antibiotic) fully and permanently reversed a severe movement disorder in horses (stringhalt graded at the worst possible score) caused by distal axonopathy with mixed polyneuropathy.
•Post-anesthetic myopathies and neuropraxias in horses are a recognized indication for topical DMSO.
•In a large clinical series of 172 horses, a DMSO-corticosteroid preparation applied to 21 conditions (including neuritis) achieved signs of improvement in 85.5% of cases.
Peripheral Neuropathies
DMSO’s therapeutic properties have allowed it to treat a wide range of peripheral nerve conditions, from complex regional pain syndrome (where it has the strongest evidence base, including multiple randomized controlled trials) to facial nerve palsy, trigeminal neuralgia, post herpetic neuralgia, compression neuropathies, diabetic neuropathy and many different types of neuropathic pain.
Complex Regional Pain Syndrome
One of my favorite therapies was discovered a century ago after observing that intravenous or locally injected procaine could almost instantaneously resolve a wide range of debilitating symptoms (or accelerate wound healing), particularly in painful scars, where the pain relief and cessation of other symptoms lasted long after the anesthetic had worn off. This led to the realization injuries (e.g., from toxins, infections, or scars) could create “interference fields” where nerves became hyper-excitable (disrupting the autonomic nervous system) and that local anesthetics could reset this, as when anesthesia wore off the hyperactive nerve, its firing pattern would reset and it would no longer be “hyperactive” (and hence no longer inappropriately trigger the autonomic nervous system).
Neural therapy’s success in treating a wide range of “incurable” symptoms led to decades of German research which mapped out how specific nerves and ganglia could contribute to specific chronic issues (while in parallel mainstream medicine recognized anesthetizing neuronal centers like the stellate ganglion had therapeutic utility). Practitioners across the world, in turn, gradually recognized how often “toxic scars” created chronic health problems and incrementally adopted the German protocols and found ways besides anesthetics to treat interference fields. Finally, the most talented ones realized that while common patterns in interference fields existed, refining their ability to detect them led to the best success, and in many cases resulted in them injecting areas outside the classic neural therapy locations.
Note: one common consequence of an interference field is chronic irritation or low grade inflammation. Another (from it driving sympathetic overactivity) is vasoconstriction, as excess sympathetic tone constricts the arterioles and blood supplying a region. This may also, in part, explain why Stanley Jacob found 50% of Raynaud’s patients fully recovered with DMSO1 and why many readers with it have reported improved circulation to their fingers and toes following DMSO.
One of the diseases many have recognized best maps to the neural therapy concept1,2,3 is “complex regional pain syndrome” (CRPS, previously called reflex sympathetic dystrophy) a chronic neurological disorder marked by severe, persistent pain—often burning, shooting, or throbbing (typically in one limb) accompanied by pain hypersensitivity and autonomic dysfunction such as skin color or temperature changes, swelling, abnormal sweating, motor dysfunction (weakness, tremors, stiffness), and trophic changes (hair, nail, or skin alterations).
The cause of CRPS is still not understood but it is recognized to typically have a trigger (e.g., a trauma, surgery, stroke, heart attack, or other injury) that is typically “much less severe” than the ensuing pain, and in some cases (CRPS Type 2) to have accompanying nerve damage.
Note: one of the side effects repeatedly linked to the HPV vaccine was CRPS Type 1.
Presently, no definitive cure exists for CRPS, so a variety of partially effective treatments are used, including secondary ones like ganglion blocks and IV ketamine (which can reset neuronal hypersensitivity and may work in cases where nothing else does). Because of this, I periodically run into patients with debilitating CRPS (which often has been there for years) who experience immediate and dramatic relief from a (correctly targeted) lidocaine or procaine injection—making it immensely frustrating that there is no conventional support for neural therapy (particularly since its uses go far beyond pain management).
Note: some psychiatric disorders are triggered by autonomic imbalances, and in CRPS (a disorder frequently associated with psychiatric co-morbidities) I have seen numerous cases where injecting a “toxic scar” with lidocaine caused longstanding mood issues (e.g., agitation or anxiety) to immediately improve. Likewise, I frequently encounter psychiatric disorders that require either addressing sources of excess sympathetic activity or deficient parasympathetic activity (e.g., one reader recently reported good effects from a DMSO protocol for the vagal nerve I shared1), while other psychiatrists I know have had significant success unconventionally using the alpha-2 agonists guanfacine and clonidine (which reduce sympathetic activity) to treat anxiety, PTSD, and panic disorders. DMSO’s use in psychiatric disorders is discussed further in the first part of this series.
Since CRPS is challenging to treat, its responsiveness to DMSO immediately caught physicians’ attention, leading to roughly a dozen clinical studies which consistently found topical DMSO cream improved acute “warm” CRPS, with the strongest effects seen when treatment begins early in the disease course.
This began with a 1985 study that transformed medical understanding of CRPS by showing that free-radical scavengers like DMSO could significantly reduce pain, swelling, and burning sensations (with an approximately 90% recovery rate when the therapy was initiated in the early stages of the illness).
In the earliest controlled studies, DMSO significantly outperformed both placebo and regional sympathetic blocks (with intravenous Ismelin) for pain reduction, range of motion, and overall clinical improvement, with one crossover study (likely unaware of DMSO’s neurological effects) concluding that DMSO’s efficacy “indicates that RSD primarily involves an inflammatory process rather than a sympathetic reflex.”1,2,3,4,5 In an RCT of 31 patients, DMSO cream reduced the median RSD-score from 5 to 0 over two months (vs. 4 to 2 with placebo, p<0.01), and in a study of 37 patients, pain scores dropped from 5.3 to 0.9 over 3.4 months Another RCT of 146 patients also found four months of DMSO was an effective treatment (approximately 80% improved with a mean 9.05 improvement on impairment score), with the greatest benefit found in warm CRPS. In a study of 74 CRPS 1 patients treated with a combination of therapies including topical DMSO, a mean 35% pain reduction was achieved after one year.1
A 145 person study compared DMSO to oral N-acetylcysteine for CRPS 1. Both treatments were effective, but DMSO was superior overall (especially in warm CRPS) and more cost-effective from a societal perspective (€2,852 vs €3,934 and better clinical outcomes).1,2,3,4 A 2012 study of 29 patients with CRPS 1 of less than one year’s duration similarly found DMSO reduced pain by 3.09 VAS points over a year, with 89.7% showing quality-of-life improvements and moderate restoration of limb function, with 12 patients who did not receive DMSO showing worse improvements.1,2 DMSO has also been incorporated into compound analgesic creams for CRPS, where 69% of patients reported pain reduction, with two achieving complete resolution (along with a case report where severe intractable CRPS 1 responded to a compound cream). Ukrainian clinicians have also reported success with overnight compresses DMSO solution mixed with dexamethasone for localized CRPS,1 and in one study, DMSO with ambroxol was found to be a highly effective CRPS treatment.
Multiple systematic reviews and German, Dutch, and Russian clinical guidelines recommend topical 50% DMSO cream for the acute inflammatory phase of CRPS (particularly for CRPS 1),1,2,3,4,5,6,7,8,9,10,11,12,13,14,15 with a standardized compounding formulation published in the Formularium Der Nederlandse Apothekers.1 DMSO has also been recommended or utilized for CRPS across numerous other clinical and rehabilitation contexts.1,2,3,4,5,6,7,8,9,10,11
Reader reports corroborate the clinical data. The most detailed CRPS report came from a reader with a multi-decade history of the condition alongside myasthenia gravis and ankylosing spondylosis, who reported that since starting DMSO in 2021–2022, they have not had a major CRPS episode: “When I can sense it returning I know what stops it.”1
Other readers have also reported significant improvements1,2,3,4,5,6,7 (e.g, “pain was gone.”1), including one reader who used topical DMSO daily for 18 years for CRPS, calling it “a freaking Miracle,”1 another CRPS in the arm and hand following a wrist fracture who’s been in remission for approximately nine years due to her veterinarian father introducing her to DMSO,1 and a reader with MS, fibromyalgia, liver fibrosis, CRPS, and lymphedema described oral and topical DMSO as “a godsend” (after about a year of use).1
Note: in rats with CRPS 1, resveratrol⬖ and ISO-1 (in DMSO) significantly improved pain thresholds and reduced inflammatory mediators and ERK1/2 signaling in the sciatic nerve, with similar results in a post-fracture CRPS model.1 An NLRP3 inhibitor in DMSO also attenuated CRPS allodynia in rats.1 In clinical practice, DMSO has also been combined with novocaine,1,2 heparin, (as Dolobene gel),1,2 NSAIDs1 and the dexamethasone and compound cream formulations described above for CRPS.
Facial Nerve Palsy
Facial nerve paralysis (Bell’s palsy) causes sudden weakness or paralysis of one side of the face, typically from inflammation and swelling of the facial nerve within the narrow Fallopian canal of the skull. While most cases resolve spontaneously, a significant minority develop permanent facial asymmetry, that fortunately, DMSO has been shown to improve.
Note: DMSO also has direct effects on peripheral nerve-mediated vascular responses, as topical DMSO produces facial flushing consistent with activation of vasodilatory nerve reflexes.
The most substantive evidence comes from a controlled study of 65 patients with Bell’s palsy, where compresses of DMSO mixed with nicotinic acid and saline were applied to the parotid region of the affected side for 10-12 sessions. Compared to conventional treatment controls, the DMSO protocol produced a statistically significant increase in the cure rate and a significant decrease in therapy duration.1,2,3
DMSO has also been used to restore mimic muscle function after peripheral facial nerve lesions by dissolving therapeutic drugs (ATP, lidase, novocaine for paretic muscles; vitamin E⬖ for spastic muscles) and introducing them into acupuncture points of the injured facial neuromuscular structures. Pretreatment involved 1-3 applications of topical DMSO followed by drug injection in DMSO solution with low-frequency electrical stimulation. In one documented case, a patient with post-cold right facial nerve paresis achieved full recovery of muscle function without residual contractures or synkinesis (involuntary movements when a different facial muscle is used due to miswiring during the nerve’s regeneration) after 10 sessions.
Several clinical guidelines and reviews recommend topical DMSO application to the facial nerve exit area during the acute period of facial neuropathy for its anti-edema, anti-inflammatory, and vasodilatory effects, positioned alongside corticosteroids, diuretics, NSAIDs, and vascular agents in the standard management algorithm.1,2,3 DMSO-containing baths and compresses are also listed as standard therapy for facial nerve neuropathies in Russian clinical practice (e.g., in a cohort of patients with facial nerve paralysis, DMSO applied at night was used as part of a multimodal protocol that successfully treated 60% of cases).
Additional applications include DMSO in postoperative dressings following composite flap surgery to correct lagophthalmos (inability to close eyelids from facial nerve paralysis), supporting anti-inflammatory care in six patients who achieved full eyelid closure.1 DMSO has also been used in iontophoretic delivery protocols for facial neuritis, where drug-impregnated wipes placed in the ear cavity and nasal passage achieved marked improvement in 93% of 154 patients with various conditions including facial neuritis.1 In patients with radiation fibrosis and secondary neuritis, DMSO was incorporated into acupuncture reflexotherapy rehabilitation protocols.1
A reader diagnosed with Ramsay Hunt syndrome (rare facial paralysis from shingles) started using DMSO and “within a week I started to see movement in my face again,” with continued improvement in taste, hearing, vision, and facial mobility.1 Another applied DMSO gel to the skin over the skull near the ear of a friend with Bell’s palsy: “He says now that it burned for a little while, then the pain subsided a lot.”1
Note: in the early vaccine literature, the nerve paralyses they caused were attributed to inflammatory edema compressing the tight pathways those nerves traveled through.1 As the facial nerve examples show, DMSO’s fluid draining properties makes it well suited for these impingements, further corroborated by Russian and Ukrainian guidelines for radiculitis and sciatica treatment using spinal DMSO and procaine compresses as a standard protocol for reducing edema and inflammation around affected nerve roots1,2,3,4
Additionally:
•DMSO mixed with novocaine is applied topically to treat post-mastectomy scalenus syndrome, a neurovascular compression that contributes to plexitis and neuropathy,1 and DMSO dissolved with B vitamins (1% thiamine chloride and 1% pyridoxine hydrochloride) has been applied to skin as part of reflexotherapy protocols for traumatic mononeuropathies and plexopathies, with positive EMG-confirmed recovery in all treated patients.1,2
•Melkerson-Rosenthal syndrome, a chronic condition characterized by macrocheilitis (swollen lips), folded tongue, and usually unilateral facial nerve paralysis resulting from impaired microcirculation of blood and lymph, has also been treated with topical DMSO-heparin ointments and heparin iontophoresis.1
•In horses, IV DMSO contributed to recovery from fourth branchial arch defects causing laryngeal paralysis, with a progressive decrease in laryngeal inflammation observed by endoscopy after intranasal DMSO-dexamethasone-nitrofurazone treatment for 5 days post-surgery.1 Non-surgical treatment of laryngeal hemiplegia induced by perivascular or perineural injection has also included topical DMSO.1 A detailed equine lameness protocol used aquapuncture injections of vitamin B12⬖ mixed with Sarapin⬖ and DMSO for treating lameness through combined acupuncture and DMSO-enhanced drug delivery.1
Note: DMSO has been used extensively for decades in horses to treat severe neurological issues (detailed here).
Trigeminal Neuralgia
Trigeminal neuralgia (TN), one of the most severe pain conditions known, is characterized by sudden, intense, shock-like facial pain along one or more branches of the trigeminal nerve. Standard treatments (carbamazepine, surgical decompression) are often only partially effective, and the condition frequently stops responding to treatment. However:
•Stanley Jacob reported on 59 patients with headaches from a variety of causes, of whom 26 out of 35 patients with TN of more than a year’s duration (many with numerous failed treatments) improved with topical DMSO, with 13 achieving a full recovery. In another early report, DMSO showed promise for TN alongside other headache types, with improvement noted in patients where topical DMSO was applied to the affected area or instilled intranasally.1,2
•A Russian patent reported “simple, effective, and free of side effects” treatment for TN: applications of napkins moistened with a solution of DMSO and 2% novocaine or lidocaine applied to the facial skin over the affected trigeminal nerve branch exits, 2–3 times daily for 20-30 minutes over 10-15 days.1 DMSO has also been recommended as part of conservative therapy for trigeminal neuralgia exacerbations via local applications, often in combination with antihomotoxic (homeopathic) preparations.1
•In patients with multiple sclerosis (experiencing TN, a recognized MS complication), topical DMSO mixed with anesthetics applied to trigger zones enabled reduction of carbamazepine to minimum doses or complete discontinuation and achievement of full remission during TN exacerbations.
•For orofacial pain syndromes involving masticatory muscle spasm, compresses of DMSO mixed with 2% lidocaine were applied to reduce muscle tone and alleviate pain as part of comprehensive management.1
•DMSO has also been incorporated into iontophoretic delivery systems for TN and facial neuritis, where electrode-wrapped sodium alginate wipes loaded with DMSO (among other agents) produced marked improvement in 93% of 154 patients.1
Note: in one small series of three patients, multiple daily applications of DMSO failed to provide any relief, though the same physician personally observed a dramatic response in a different patient treated by Stanley Jacob (suggesting TN treatment requires the correct DMSO protocol).
Reader reports of trigeminal neuralgia responding to DMSO were among the most dramatic I received. One reader’s mother had been in “almost constant pain for years” with TN so severe she could not speak clearly, sing, or eat many foods. After starting daily DMSO on the back of the neck, “the pain was gone by the evening. That was three weeks ago and she has not had a flareup since.”1 A reader’s wife with MS-related secondary trigeminal neuralgia (painful for over a year and a half) tested DMSO cream on a small spot on her face: “her pain dropped 90%. The next morning she put it all over the trigeminal area, and the pain is 99.9% gone. Even after three days without reapplication, the pain hasn’t come back.”1 Another reader used DMSO on a TN flare and reported “80% resolved…I can manage the rest!”1
Other readers also reported TN relief,1,2 including one who had tried DMSO for tinnitus and then discovered it also treated their recently diagnosed cervical spondylitis, with TN-like symptoms resolving in 3–5 days.1 One reader with vascular EDS and 18 years of TN and facial neuropathy reported success using DMSO on the face near the ear.1
Note: a Russian literature review noted that treatment of trigeminal neuritis with DMSO is “long-term, from 1 to 6 months.”1
Additionally, readers with occipital neuralgia have reported success with DMSO1,2 (e.g., one who’d tried many treatments including nerve blocks experienced “amazing improvement” from DMSO).
One reader with superior oblique myokymia (a rare condition causing one eye’s visual field to jump, occasionally producing dangerous double vision while driving that often following TBIs that subsequently compress the nerve) found that 10% DMSO in distilled water used as an eye drop “does work to temporarily hit the off switch. It hasn’t cured it, but it’s reassuring to have an actual tool in the toolbox.” The condition had been deemed untreatable by the pre-eminent neuro-ophthalmologist in the country.1
Combination Studies
A variety of agents dissolved in DMSO have shown benefit in TN models. A JAK/STAT3 pathway inhibitor (AG490) increased mechanical sensitivity thresholds (decreasing pain) and reduced phosphorylated STAT3 and glial activation. A protease-activated receptor 1 inhibitor (SCH79797) modulated orofacial pain thresholds in a chronic compression model. Intrathecal atypical antipsychotics (aripiprazole, quetiapine, olanzapine) produced dose-dependent reductions in mechanical allodynia in a trigeminal neuropathic pain model. A P2X4R antagonist relieved TN pain in rats via p38/BDNF inhibition. Melatonin⬖ reduced TMJ osteoarthritis chronic pain via MT2 receptors in trigeminal ganglion neurons.
Note: TNF-a signaling (which DMSO suppresses) has been shown to contribute to mechanical hypersensitivity in masseter muscle during temporomandibular joint inflammation (which is often linked to TN).1
A DMSO gel formulation (with sodium carmellose) was specifically developed and tested for conditions including TN, showing stable anti-inflammatory efficacy comparable to standard DMSO ointments (reducing kaolin-induced edema by approximately 63-74% at 5 hours) with superior convenience and no toxicity.
Post-Herpetic Neuralgia
DMSO has consistently demonstrated significant efficacy against herpes simplex and herpes zoster (shingles) infections, with numerous studies (detailed here) and reader reports I’ve received showing DMSO consistently reduced pain and significantly accelerated disease resolution (which frequently was miraculous for readers).
Note: for treatment of acute herpes, DMSO worked better in combination with idoxuridine (IDU, an antiviral which only worked if DMSO transported it through the skin). While this combination worked and was approved in Europe (e.g., as Herpid or Zostrum), acyclovir (which, while potentiated by DMSO did not require DMSO for delivery) was discovered not long after and displaced it—which is unfortunate, as while acyclovir is helpful, there are many herpes simplex and shingles cases that acyclovir alone does not sufficiently address.
In addition to treating herpes infections, DMSO also addresses the neurological complications they create (e.g., consider the previous Ramsay Hunt syndrome report where a reader successfully treated this challenging condition1). Likewise:
•Facial (trigeminal) herpes zoster—the form of shingles most likely to progress to postherpetic neuralgia if untreated—responded well to DMSO-IDU: pain duration was significantly shortened (median 13 days vs. 1–3 months in controls), pain persisting beyond 30 days in only 30% vs. 82%, with faster scab formation and less fever.1,2
•In a case series of 45 shingles patients, William Campbell Douglass reported that 79% had a “good” response and 14% had a fair response to DMSO. Of the 13 acute cases with concurrent neuralgia, 10 had a good response and 3 had a fair response.
Post-herpetic neuralgia (PHN, persistent nerve pain after shingles resolves) is one of the most debilitating complications of shingles, disproportionately affecting patients over 60 and frequently does not respond to standard treatments. Fortunately, DMSO has shown consistent benefit for PHN across both prevention and treatment, with several clinicians finding it superior to other available options for chronic cases.
The most striking finding is that DMSO appears to largely prevent PHN when used during acute shingles. At a 1980 Congressional Hearing, Dr. Scherbel of the Cleveland Clinic testified that with DMSO application during acute shingles, they never saw post-herpetic neuralgia follow.1 This was corroborated by a 1992 RCT of 171 patients showing topical 40% IDU (an antiviral) in DMSO was superior to acyclovir in preventing PHN development, and a 1974 RCT of 118 patients finding the combination significantly improved post-herpetic neuralgia outcomes.1,2,3 Earlier controlled studies similarly showed that both 5% and 40% IDU in DMSO dramatically reduced pain duration (patients were “delighted, for the pain disappeared within a median of two days”), with 40% IDU producing the strongest results.1 Finally, a pooled analysis of controlled studies found that while acyclovir and corticosteroids showed no significant preventive effect on PHN, IDU in DMSO indicated possible benefit.1
Note: Stanley Jacob noted that while the FDA was stonewalling DMSO, DMSO plus IDU was an approved topical prescription in England and Ireland. Sadly, it is still not available in North America.
For established PHN, DMSO also shows benefit. In a large study of patients with various conditions being treated with DMSO, 6 of 9 PHN cases achieved complete remission within 2 months, with 2 achieving partial remission.1 A German study reported positive results in 10 of 11 shingles and PHN cases,1 and in Douglass’s case series of 22 PHN patients, 18 had a good response and 2 had a fair response.1,2 One physician with extensive personal experience noted that “in post-herpetic neuralgia, particularly that which is chronic, pain relief is more striking with topical DMSO than with any other type of treatment,” and Stanley Jacob likewise reported successfully treating chronic PHN that had been present for over 2 years.1,2 The Pain Center at Mount Sinai Medical Center (circa 1980) similarly used DMSO for PHN cases that had not responded to other therapies.1
DMSO-based combinations have further improved herpetic neuralgia:
•In 25 PHN patients, topical 40% DMSO with dyclonine and dexamethasone (applied 2-3 times daily, combined with oral B vitamins and mecobalamin) relieved pain within approximately 10 minutes, with significant improvement in 5 days and marked reduction after 2 weeks.1
•In 31 PHN patients, a (unspecified) topical Chinese herbal medicine combined with DMSO significantly reduced McGill pain scores and improved quality of life compared to 29 patients receiving standard Western medicine,1 with 80 additional cases treated similarly.1
•A complement-inhibiting formulation containing DMSO and glutaraldehyde produced rapid disappearance of acute herpetic neuralgia and accelerated remission of local symptoms, with the mechanism attributed to inhibition of local anaphylatoxin release.1
•A severe case of trigeminal ganglionitis from herpes zoster (complicated by keratitis and cerebral vasculitis with hemiplegia) was treated with DMSO applications to scar areas as part of comprehensive therapy, contributing to pain management and reduced post-herpetic scar size at one year.1
•One reader with three years of PHN reported DMSO and Frankincense, upon the first application, stopped all pain.1
Compression Neuropathies
Compression neuropathies (tunnel syndromes) occur when peripheral nerves are compressed within anatomical tunnels, causing pain, numbness, weakness, and progressive nerve damage. The most common are carpal tunnel syndrome (median nerve at the wrist) and cubital tunnel syndrome (ulnar nerve at the elbow), but compression can affect nerves throughout the body including the sciatic nerve (piriformis syndrome) and upper extremity plexus (scalenus syndrome). Like the previously discussed nerve compressions, these also respond to DMSO:
•Multiple Russian clinical guidelines recommend DMSO-novocaine applications for tunnel neuropathies, with gauze pads soaked in the mixture applied daily for 4-6 hours over 7-10 procedures.1,2,3,4
•In a 2008 study of patients with carpal and cubital tunnel syndromes in diabetes, topical applications of DMSO and 2% novocaine (gauze dressings applied for 40-60 minutes daily over 14 days) produced clinical improvement: 13.8% of affected hands showed significant improvement (primarily carpal tunnel), 69% showed slight improvement with reduced pain and paresthesia, and minor EMG improvements in distal latency were observed. Notably, unlike corticosteroid injections (the gold standard for non-diabetic patients), DMSO-novocaine applications had no impact on blood glucose levels, making them particularly suitable for diabetic patients.
•DMSO has been successfully combined with corticosteroids to treat carpal tunnel syndrome (which one study reported reduced pro-fibrotic gene expression in carpal tunnel fibroblasts1). Likewise, Russian occupational health guidelines also recommend DMSO compresses (combined with analgesics, hydrocortisone, or lidocaine) for prevention and treatment of carpal tunnel syndrome in workers with prolonged computer use.1 Finally, a photodynamic protocol utilizing DMSO mixed with a photosensitizer (prior to laser irradiation) achieved pain elimination in 70% and overall efficacy in 90% of 50 patients.1
Note: DMSO has also successfully treated carpal tunnel syndrome caused by amyloidosis1,2 with electron microscopy confirming DMSO ruptured and dissolved the compressing amyloid fibers.1
•For piriformis syndrome (sciatica), DMSO compresses mixed with anesthetics and glucocorticoids were applied for 20-30 minutes to the area of nerve compression.1,2
A more detailed differentiated protocol for subpiriform sciatic neuropathy (distinguishing four clinical variants by predominant nerve involvement) applied DMSO with novocaine topically on the gluteal region and along the sciatic nerve path, alongside piriformis blocks, muscle relaxants, and magnetolaser therapy, achieving superior pain reduction on VAS scores (e.g., from 71.4 to 20.2 versus 36.2 with standard therapy) and improved muscle strength and EMG parameters.1
•A retrospective case series of 11 patients with compression-ischemic radial neuropathy used topical DMSO combined with hyaluronidase novocaine applied in compresses alongside systemic medications and pain-free rehabilitation. Over a median 12-week follow-up, mean pain decreased 69.1% (VAS from 6.8 to 2.1, p<0.001), muscle tone improved from Modified Ashworth Scale 3 to 1, and active wrist extension recovered in 72.7% (with stronger results in injuries less than 6 months old). Local skin irritation occurred in 27.3%.1,2
Readers with carpal tunnel syndrome consistently reported relief from DMSO. Several described rapid results: one found it “helped my carpal tunnel wrist pain immediately,”1 another reported “no pain after 2-3 days,”1 and a third called it “Miraculous!”1 A retired chiropractor with advanced degenerative changes in the carpometacarpal joint (from 27 years and over 250,000 patient visits) who had refused oral anti-inflammatories due to unacceptable risk-benefit ratios reported “nearly 100% improvement” in pain and soft tissue swelling from topical DMSO applied at bedtime.1 Multiple readers described long-term management: one who had crocheted for years used DMSO “when needed” on wrists and thumbs,1 another used it nightly on hands and wrists for carpal tunnel and arthritis,1 and a reader with carpal tunnel symptoms (tingling in the right hand from cervical spine pathology) found improvement from applying DMSO to the upper back and cervical spine, though “not as quickly as the thumb.”1 One reader’s son used it on his wrist for carpal tunnel “with good results,”1 and another with “the most horrible pain” from carpal tunnel (whose surgery had been postponed) “got it controlled with the DMSO.”1 Another applied DMSO to the healing surgical wound after carpal tunnel release, with results “much further ahead than comparable surgical wound progression.”1 A reader with plantar fasciitis, carpal tunnel, and multiple other conditions (including CRPS and myasthenia gravis) as part of a complex autoimmune presentation reported improvement in all since starting DMSO.1 Other readers also reported carpal tunnel relief.1,2,3,4,5,6,7
For piriformis-related sciatic compression, readers found that topical DMSO combined with CBD oil and castor oil or peppermint oil and lidocaine cleared the pain.1,2,3 Bursitis of the shoulder (a common impingement-related compression) responded to DMSO in multiple reports, with one reader whose doctor and physiotherapist “were trying to force me into a treatment that didn’t sit well” finding that one month of a DMSO mix was “a miracle” for a frozen shoulder with bursitis and an impacted nerve in the neck.1
Note: shoulder bursitis was one of the very first conditions DMSO was recognized to treat, and as a result, a large number of studies (and reader reports1,2,3,4,5,6,7,8,9,10,11,12,13,14,15) corroborate this. Likewise readers have reported significant improvement for other bursitis (most frequently of the hip, but also other areas like the knee and foot).1,2,3,4,5,6,7,8,9,10, 11,12,13,14,15,16,17,18,19,20,21,22,23,24
DMSO has also been used for leprosy neuritis (in the hypertrophic form), where 25% DMSO mixed with lidase was applied via magnetophoresis as part of comprehensive physiotherapy aimed at reducing pain, inflammation, and fibrosis, and improving nerve conduction (while separately DMSO combinations also healed nerves damaged by leprosy1) . A clay-based balm (Kavalgin) incorporating DMSO as a penetration enhancer alongside propolis and laurel essential oil was patented for treating neuritis, neuralgia, osteochondrosis, and sciatica.
Autoimmune Neuritis
In experimental autoimmune neuritis (EAN, an animal model of Guillain-Barré syndrome), a prostaglandin E2-EP4 receptor antagonist (L-161982) dissolved in DMSO repeatedly delayed disease onset, reduced peak clinical scores, decreased inflammatory cell infiltration (IFN-γ, IL-17, TNF-α, IL-6), suppressed lymphocyte proliferation, and reduced chemokine expression (CXCL-12, MCP-1) in sciatic nerves, with immunization-phase treatment superior to onset-phase treatment.1,2,3,4 Notably, in a study of 11 patients with IgM monoclonal gammopathy-associated demyelinating polyneuropathy, the sole individual lacking detectable anti-myelin autoantibodies was the one previously treated with DMSO.
Additionally, DMSO has been repeatedly shown to address encephalitis and encephalomyelitis from a variety of causes including autoimmunity (detailed here), with one reader reporting it cured an incurable case,1 while one reader with Morvan’s syndrome, a rare and severe autoimmune channelopathy (that developed following viral encephalitis) reported that after two weeks of topical 70% DMSO cream, inflammation in his hands visibly decreased and pain was reduced by 75%. His case was particularly severe, having required multiple nerve decompression surgeries, four joint replacements, cervical fusion, and two nerve stimulator implants.
Myasthenia Gravis
In order for skeletal muscles to fire, they need to receive acetylcholine from the nerve that directs them. In myasthenia gravis (MG) the body forms antibodies to the muscle’s acetylcholine receptors (AChRs), and as they are destroyed, the muscles need more and more acetylcholine to be sent by the nerves to activate. MG is hence managed by various immune-suppressing medications, filtering the AChR antibodies out of the blood, and acetylcholine esterase inhibitors (which boost acetylcholine levels)—suggesting DMSO’s anti-inflammatory and AChR-augmenting properties (via acetylcholine esterase inhibition) may benefit the disease.
DMSO’s potential for MG was initially discovered (accidentally) in 1980, when two researchers tested a variety of agents for their ability to reduce AChR antibodies, and realized that the DMSO being used as a vehicle for the various agents they were testing was independently reducing those antibodies. They then found that giving rats daily intraperitoneal injections of 1 mL DMSO for two weeks resulted in a 52% decrease in AChR antibodies (but not total IgG levels) that persisted for an additional six weeks after treatment was terminated.1,2
Note: after this discovery, the researchers expressed their eagerness to test DMSO in humans with MG (the New York Times even covered it).
A follow-up rat study then found DMSO suppressed anti-AChR antibody levels by an average of 53%–76%, with the effect being similar regardless of whether DMSO was given orally, rectally, or intraperitoneally. Additionally, DMSO treatment suppressed the anti-AChR antibody response to a weak primary antigenic stimulus. Interestingly, when given during strong primary or secondary immune responses, DMSO instead enhanced antibody production 1.7–2.8-fold — indicating bidirectional immune modulation depending on timing and stimulus strength (or DMSO’s ability to potentiate allergens).
These antibody findings were complemented by direct evidence that DMSO restores neuromuscular function. In ex vivo mouse nerve-muscle preparations where tubocurarine was used to mimic MG (reducing the strength of nerve-evoked muscle contractions), DMSO produced a rapid, dose-dependent, and sustained restoration of twitch force — with 0.1% restoring 20–30% of force and 0.75% achieving complete restoration that was sustained for over 150 minutes. Electrophysiology confirmed DMSO increased the amplitude of nerve signals at the muscle by ~25–30%, consistent with its acetylcholinesterase-inhibiting properties.
Additional studies in frog and mammalian nerve-muscle preparations confirmed that DMSO at concentrations ≤1% enhanced neuromuscular transmission through acetylcholinesterase inhibition, while concentrations above 1% began to have depressant effects in mammals, and that THC (but not CBD) counteracted this restoration of neuromuscular function.1,2,3,4 DMSO has also been shown to reverse neuromuscular blockade caused by organophosphates (which poison the same acetylcholinesterase system that is therapeutically targeted in MG).1,2,3,4,5,6,
Note: this research inspired a 1982 study to determine if DMSO suppressed thyroid autoantibodies (which were experimentally induced in rats). It did, and also was found to increase the ratio of IgM to IgG plaque forming cells (which suggested a true immunoregulatory effect). In turn, some patients report that DMSO benefits autoimmune thyroiditis.
A variety of agents combined with DMSO have also shown benefit in experimental autoimmune MG models — including resveratrol⬖ (which reduced anti-AChR antibodies and protected AChR density at the neuromuscular junction), total glucosides of peony⬖ and artemisinin⬖ (both reduced clinical scores and anti-AChR antibodies while modulating regulatory T cells), atorvastatin-derived exosomes,1,2,3 and a caspase-1 inhibitor (which suppressed disease progression via IL-1β/IL-17 pathways).
Separately, sepsis-induced disruption of acetylcholine receptor clustering on muscle cells was reversed by GSK3β inhibition, restoring the receptor aggregation needed for normal neuromuscular transmission.1,2 In a rat sepsis model, rapamycin similarly improved nerve conduction velocity, muscle action potential amplitude, and survival by restoring acetylcholine receptor homeostasis.
Sadly, while physicians have highlighted DMSO’s potential for human patients, no human studies have ever been performed for DMSO with MG. However, one reader with generalized MG reported that after starting oral and topical DMSO in 2022, her muscle fatigue, cognitive function, and vision dramatically improved, and she has not had a myasthenic crisis since. She noted that higher doses at night would wake her after an hour feeling alert and functional — which she attributed to DMSO boosting her acetylcholine levels — and described the effect as “better than the pyridostigmine I used to take 6x/day.” Another reader with generalized MG alongside multiple other autoimmune conditions reported no myasthenic crises since starting DMSO in 2022, along with dramatically reduced muscle fatigue, greatly improved cognition and near-normal vision — after having been on 30 prescription medications, she is now nearly off all of them1,2 while a third reported “such amazing results” including “my swallowing and speaking goes back to normal” and “right side facial grimace reducing.”1,2
Diabetic Neuropathy
Diabetic peripheral neuropathy is one of the most common (and challenging) complications of diabetes, affecting up to 50% of patients and causing progressive sensory loss, pain, and weakness that frequently leads to foot ulcers and amputations. Fortunately, DMSO’s therapeutic mechanisms are well suited to addressing it (without affecting blood sugar like conventional corticosteroid treatment1) and many readers have shared profound improvements for diabetic neuropathy.
As such, DMSO has been considered as a treatment for diabetic hand syndrome (which can include scleredema, sclerodactyly, and Dupuytren contractures involving both neuropathic and vascular components).1 For example, in a clinical study of 250 diabetic patients (88 with tunnel neuropathies, often comorbid with diabetic polyneuropathy), DMSO applications with novocaine were recommended to improve blood flow and reduce edema, though the primary therapeutic focus in that study was Tiogamma⬖ (intravenous alpha-lipoic acid), which showed superior overall efficacy.1,2
A substantial body of preclinical research has used DMSO to deliver agents targeting the specific pathways disrupted in diabetic neuropathy. Multiple studies in diabetic Schwann cell and mouse models found that HDAC inhibitors (trichostatin A⬖) upregulated DCXR expression, increased nerve growth factor, and improved peripheral nerve function including mechanical and thermal thresholds, with the therapeutic mechanism operating through HDAC5/DCXR signaling. High glucose was shown to upregulate DNMT1 expression, increase BDNF promoter methylation, and reduce BDNF in Schwann cells (with the DNMT inhibitor 5-Aza-2’-deoxycytidine reversing this suppression), while diabetic mice showed reduced sciatic nerve BDNF and myelin abnormalities. NF-κB inhibition restored autophagy in high-glucose Schwann cells by increasing Rab5 expression. Trichostatin A⬖ restored autophagy in high-glucose Schwann cells, increasing the LC3-II/LC3-I ratio by 1.6- to 1.74-fold.
Exogenous BDNF delivered intrathecally significantly elevated pain thresholds and inhibited hyperexcitability of dorsal root ganglion neurons in diabetic neuropathy rats (effects blocked by TrkB-Fc pretreatment). In chronic diabetic itch, a P2Y12 antagonist alleviated thermal and cold hyperalgesia and improved sciatic nerve conduction velocity.
Additional agents showing neuroprotective effects in diabetic neuropathy models include allopregnanolone (inhibited caspase-3, decreased the Bax/Bcl2 ratio, and prevented PC12 cell apoptosis from high glucose while ameliorating thermal hyperalgesia in diabetic rats), resveratrol⬖ (increased Nrf2 expression, inhibited NF-κB, reduced peripheral nerve apoptosis, and improved pain and temperature sensitivity), and phloretin⬖ (improved behavioral outcomes and sciatic nerve antioxidant status while reducing inflammation).
Finally, in diabetic cardiac autonomic neuropathy, Ferrostatin-1 and P2X7 inhibitors (e.g., hypericin⬖) reduced heart rate abnormalities, sympathetic discharge frequency, cardiac injury markers, and ferroptosis indicators.
Chemo neuropathy
In chemotherapy-induced peripheral neuropathy, berberine⬖ prevented paclitaxel-induced neuropathy in rats by improving pain thresholds, reducing sciatic nerve oxidative stress, and enhancing Nrf2 gene expression.
Likewise, DMSO, used as a transdermal delivery enhancer significantly enhanced the antihyperalgesic effect of hyaluronan⬖ , reducing both prostaglandin E2 hyperalgesia and chemotherapy-induced peripheral neuropathy, with prolonged effects upon repeated application.
Vibrational Disease
Vibration disease is an occupational condition caused by prolonged exposure to local vibration (typically from power tools), resulting in vascular, nerve, and musculoskeletal damage in the upper extremities.
In patients with vibration disease, DMSO water solution applied as skin compresses to affected upper extremities for 1–1.5 hours daily over 12–15 procedures produced positive effects in most cases of regional angiodystonia (impaired circulation) and sensory or autonomic polyneuropathy, with partial benefit for muscle dystonia (spasms) and stiff or frozen shoulders. The technique simplified therapy by eliminating physiotherapy procedures and reducing or eliminating the need for medications, lowering both treatment costs and clinical course duration.1,2 DMSO was also used as a topical agent for vibration disease in Chinese clinical practice, leveraging its analgesic, anti-inflammatory, vasodilatory, microcirculation-improving, and immunosuppressive properties.1
Peripheral Neuropathy Reader Reports
Many readers reported that peripheral neuropathy (from a wide range of causes) responded to DMSO, with relief typically beginning within one to several days after topical application to the affected area (most commonly the feet) and responses ranging from partial improvement to near-complete resolution.
Diabetic Neuropathy
A type 1 diabetic with burning, itching leg pain (suspected neuropathy and nerve damage) found that a gel made their “legs feel a whole lot better.”1 Another with type 2 diabetes who had gotten their A1C from 11.4 to 5.0 but still had lymphedema and neuropathy started DMSO: “I had lost about 80% of feeling from my knees down. I now have about 85% feeling in my legs and feet.”1 Another reported DMSO “has resulted in FEELING RETURNING to the feet!!!!”1 A reader used DMSO cream on their feet at night; tingling improved by day one, and by the fourth morning “all the purple mottling was completely gone.”1 Additional readers with diabetic neuropathy reported pain reduction and restored sensation.1,2,3,4,5,6
After the first few [topical] applications, [my husband] began to get feeling back in his feet. This, after 9 years of basically numb feet.😳1,2
Vaccine-Injury Neuropathy
A reader developed acute inflammatory demyelinating polyneuropathy (on the Guillain-Barré spectrum) eight days after the Shingrix vaccine, leaving them with painful foot spasms and numbness for five years. Topical DMSO eliminated the spasms from the first night of use.1,2 Another developed peripheral neuropathy in the feet within weeks of the Pfizer booster and has been using 70% DMSO with castor oil twice daily for six months with “slow steady improvement.”1 The reader who reported the Moderna vaccine injury (gastroparesis, brain fog, SFN, MCAS, POTS, tinnitus, insomnia) described all symptoms “improving for the first time in 3 1/2 years” with DMSO.1
Chemotherapy-Induced Neuropathy
A reader with chemotherapy-induced neuropathy used DMSO on the feet and reported elimination of neuropathy within two weeks of daily application (compared to the back pain that resolved with a single application).1,2 Another with neuropathy in hands, feet, and face from immunotherapy found significant improvements.1 Finally, one reported shooting pains from peripheral neuropathy (from chemo 10 years prior) were controlled with nightly DMSO foot wraps or oral DMSO at bedtime.1,2,3,4
Other Neuropathies
A reader with idiopathic neuropathy for 20 years noticed more feeling in the feet and less numbness after beginning DMSO.1 One was “facing foot surgery to remove damaged nerves” and walking was “EXCRUCIATING”; three weeks of DMSO with red light therapy twice daily “HEALED my nerves. No more pain, no surgery needed.”1 A reader with small fiber neuropathy found the DMSO roll-on provided relief on the bottom of the feet1 while another used it for nerve damage in the hips from Lyme disease.1 Numerous additional readers reported neuropathy improvements in the feet,1,2,3,4,5,6,7,8,9,10, 11,12,13,14,15,16,17,18,19,20, 21,22,23,24,25,26,27,28,29,30, 31,32,33,34,35,36,37,38,39,40, 41,42,43,44,45,46,47,48,49,50, 51,52,53,54,55,56,57,58 shins,1 hands,1,2,3 arms1 and legs1,2,3,4,5,6,7 (or unspecified areas 1,2,3,4,5,6,7,8,9,10, 11,12,13,14,15,16,17,18,19,20, 21,22,23,24,25,26,27).
A reader shared 50% DMSO applied to the legs of a friend’s daughter born with Charcot-Marie-Tooth disease (a hereditary demyelinating neuropathy characterized by absent myelin sheath, painful leg bending, and buckling when standing) gave her immediate relief from the first application.1
The most visually striking report came from a reader whose 85-year-old mother’s toes and ankles had turned “a blackish blue color” from neuropathy, with nightly toe curling and cramping. After three weeks of daily DMSO, “the normal color has returned to her feet and legs. She has not had a cramp since the very first day of DMSO and she now has feeling back in both of her heels.”1
Note: several readers noted that long-standing neuropathy improved more slowly than acute conditions, with some requiring weeks to months of consistent application,1,2,3 while a few with very long-standing neuropathy reported only partial improvement.1,2 One reader observed that while topical DMSO helped, switching to oral administration produced further benefit.1,2,3
Neuropathic Pain
Medical management of pain typically revolves around identifying the pain generator and providing a medical therapy (e.g., an anti-inflammatory or opioid) which is known to temporarily counteract the type of pain present. While this model is sometimes quite useful (e.g., it can be used to identify emergency conditions like appendicitis which require immediate treatment, prevent permanent sensitization from a severe acute injury, or offer relief when the underlying cause is untreatable), it frequently results in patients needing to take increasingly toxic doses of partially effective pain medications.
Note: this helps explain why, from the start, the most popular use for DMSO was pain management, as it was able to safely address a wide range of pain conditions conventional therapies often could not improve (e.g., DMSO use for cancer pain is discussed here), and likewise why, sixty years later, the most popular article in this series was on DMSO’s uses for treating pain or why the most common testimonial I receive from readers was DMSO addressing some type of (often debilitating) source of pain nothing else had worked on. Sadly, despite immense needs for effective pain therapies (e.g., due to the opioid crisis), DMSO has languished in obscurity, something I believe boils down to pain management being one of the most reliable markets in medicine, and hence something many parties would not want to be displaced by an essentially free alternative.
From a young age, I was able to feel others’ pain, and in medicine, this caused me to gravitate towards a functional perspective on treating pain where, I would focus on why a pain generator caused pain, and then try to either directly address the pain generator or the process it triggered which caused pain. Because of this, while studying DMSO, it immediately jumped out to me that many of DMSO’s mechanisms overlapped with the mechanisms of the approaches I would use to treat pain, but rather than strongly affecting one process, it would instead have a diffuse effect on a variety of processes, thereby making it a safe (not too strong) “DIY” therapy individuals could often use at home without requiring the precise targeting many of the modalities I used required (while conversely, in a subset of pain cases, that targeting or a stronger therapy than DMSO was needed). For example DMSO:
•As described above, resets hypersensitive neural circuits.
•Relaxes muscles (which, when tight, are often a root generator of pain)
•Increases arterial, venous, and lymphatic circulation (also often a root generator of pain when dysfunctional)
•Is a powerful anti-inflammatory, edema reducing and free radical scavenging agent (addressing another major subset of pain).
•Heals injured tissues (addressing another major subset of pain—nociceptive pain).
One of the most challenging types of pain to treat, neuropathic pain arises from a lesion or disease of the somatosensory nervous system and is often characterized by burning, shooting, or electric-shock sensations with heightened sensitivity to touch and temperature. A closely related and equally difficult condition is nociplastic pain, which stems from altered nociceptive processing without clear tissue damage or nerve lesions, yet shares many of the same features and treatment resistance. In both cases, conventional analgesics often fail, and analgesic options such as anticonvulsants, antidepressants, and opioids typically provide only partial relief with significant side effects (e.g., the issues with the seizure drugs gabapentin and Lyrica are discussed here). DMSO, however, has consistently shown remarkable benefit for these pain states. This I attribute to it:
- Resetting hypersensitive nerve circuits that trigger and maintain pain sensitization.
- Restoring blood flow to nerves (improving endoneurial microcirculation, a key driver of neuropathic pain when impaired).1,2
- Improving fluid balance inside nerves by reducing swelling and pressure while supporting axoplasmic flow.
- Relieving compression on nerves (e.g., from tight muscles or edema).
- Promoting actual healing and regeneration of damaged nerves1,2 (thereby reducing ectopic firing and hypersensitivity that generate neuropathic pain).
- Scavenging inflammatory free radicals that damage nerves and generate neuropathic pain.1,2
- Enhancing the body’s own pain-relieving systems (including stabilizing natural opioids like enkephalins and reducing pain transmitting substance P in the spinal cord).
- Balancing autonomic tone by reducing sympathetic overactivity and increasing parasympathetic activity via direct nerve-modulating effects and acetylcholinesterase inhibition (which is known to reduce postoperative pain, neuropathic pain, cancer pain, and chronic pain with opioid-sparing effects1,2,3,4).
Note: in Merck’s early trials, the one type of pain DMSO did not help was psychiatric pain, though given that psychiatric disorders can worsen existing pain (e.g., by increasing sympathetic tone, arteriolar constriction, or muscle contraction), DMSO could potentially reduce the psychiatric exacerbation of pain (although this area remains largely unstudied).1 - Selectively blocking the transmission of neuropathic pain signals.
- Allowing other therapeutic agents to be delivered directly to sites of neuropathic pain (e.g., 5% DMSO hydrogels were shown to facilitate permeation of gabapentin across human epidermal membranes, potentially enabling topical delivery for peripheral neuropathic pain and thereby bypassing the systemic complications of oral gabapentin and a Russian patent using a selective M1 inhibitor for topically treating neuropathic pain without weakening perception of normal stimuli.1).
Note: Safranal⬖ in DMSO produced significant analgesia mediated entirely through the GABAergic pathway (unaffected by naloxone), confirming the existence of opioid-independent analgesic mechanisms accessible through DMSO-delivered natural compounds.1
As many of these (e.g., circulatory improvements and healing of nerves) were discussed in the first and second parts of this series (or previously in this article), I will now focus on a few of DMSO’s pain reducing mechanisms that were not previously discussed and specifically relate to neuropathic pain and nociplastic pain.
Note: I believe a significant portion of nociplastic pain results from brain tissue injury (e.g., a loss of blood flow to pain-dampening regions or direct compression of brain tissue). Many of the mechanisms listed above also operate in the brain (e.g., Russian researchers extensively demonstrated DMSO’s ability to reduce the brain tissue injury and functional loss resulting from chronic stress).
Preventing Pain Transmission
Many different nerve fibers exist in the body. One group, known as the “small fibers,” is responsible for transmitting specific sensations. In particular, C fibers are frequently linked to debilitating chronic pain syndromes. For example, in small fiber neuropathy they commonly produce sensations of pins-and-needles, pricks, tingling, and numbness alongside burning pain and electrical shocks, while in nociplastic pain C fibers transmit slow, diffuse, dull, aching, or burning sensations.
Note: the five most common symptoms of COVID vaccine injuries, in order, are fatigue, post-exertional malaise, brain fog (discussed further here and here), small fiber neuropathy, and dysautonomia.
Due to DMSO affecting nerves in a biophysical manner, at therapeutic concentrations it selectively blocks the conduction of small nerve fibers1 (the C fibers) while not affecting larger nerve fibers1 thereby allowing it to address neuropathic pain without altering the other functions of the nervous system (which may explain why rather than developing a resistance to it, chronic pain patients often find DMSO’s efficacy increases over time). Specifically:
•In cat sural nerves, 5% DMSO slowed C fiber conduction velocity and decreased amplitude, 9% blocked conduction entirely, and the block was instantaneous at 15%, with all effects reversing once DMSO was washed off.1,2
•In cat radial nerves, lower concentrations selectively blocked C fibers and then Aδ fibers (the two fiber types responsible for pain transmission), while higher concentrations were required to affect the larger Aβ and Aγ fibers, with 5-10% DMSO also blocking C-fiber afterdischarges (a process associated with painful stimuli).1 At much higher concentrations (75–100%), this preferential pattern persisted and was reversible if washed off early.1
•In isolated frog sciatic nerves, 6% DMSO significantly slowed conduction velocity (which reversed once the nerves were washed).1
Note: this author concluded the conduction blocking was likely due to mechanisms such as cholinesterase inhibition rather than direct nerve blockade.
•One detailed review found DMSO’s analgesic effects lasted approximately 6 hours (compared with 2 hours for morphine), and intrathecal (into the CSF) 50% DMSO produced 30 minutes of complete anesthesia in cats with full recovery. The same review confirmed that 5-10% DMSO rapidly blocked pain-conducting C fibers and that 6% DMSO reduced sciatic nerve conduction velocity by 40%.1
These nerve-blocking properties suggest DMSO could be combined with natural substances that independently block nerve conduction. In isolated frog sciatic nerves, various aroma oil compounds dissolved in DMSO concentration-dependently and reversibly inhibited compound action potentials through mechanisms independent of TRP channel activation, with linalyl acetate⬖ showing efficacy comparable to lidocaine, ropivacaine, and cocaine, and linalool,⬖ citral,⬖ and citronellal⬖ also demonstrating significant blocking activity.1 Capsaicin and related vanilloid compounds⬖ (including eugenol⬖ and dihydrocapsaicin⬖) similarly blocked nerve conduction independent of TRPV1 activation, through direct sodium channel blockade with potency determined by the hydrophobic side chain length.1 Likewise, Kampo herbal formulations (particularly daikenchuto,⬖ containing processed ginger, ginseng, and Japanese pepper) concentration-dependently inhibited nerve conduction (~70% reduction at 2 mg/ml) partly through plant-derived TRP agonists (piperine,⬖ cinnamaldehyde⬖) but also through TRP-independent mechanisms, with 1% DMSO alone having no effect on compound action potentials.1,2
Note: an insect study found DMSO preferentially inhibits peripheral sensory receptor activity over axonal conduction: in a proprioceptive organ, DMSO blocked sensory neuron responses to mechanical stimulation at just 0.85% (50% block in 18-20 minutes), while blocking sensory axon conduction required roughly five times higher concentration (4.6%), demonstrating sensory receptor inactivation as a distinct analgesic mechanism separate from C fiber conduction block.1
Receptor and Ion Channel Modulation
DMSO suppresses NMDA and AMPA induced ion fluxes in neurons, each of which are receptors linked to chronic pain (e.g., NMDA is linked to central pain sensitization),1,2 a property I believe may partly account for why DMSO treats complex regional pain syndrome and which has also been proposed to explain its utility in treating cancer pain.1,2
Like local anesthetics, DMSO has also been observed to block sodium and calcium ions’ entry into cells, which has been proposed to explain how DMSO can help cancer pain.1,2 Likewise, in whole-cell voltage-clamp studies on differentiated neuroblastoma × glioma hybrid cells, DMSO (0.5–1%) reversibly blocked voltage-gated Na⁺, K⁺, and Ca²⁺ currents, with effects resembling those of local and general anesthetics.1
Finally, detailed electrophysiological studies in unmyelinated neurons confirm that DMSO blocks nerve impulses at approximately 8–15% concentrations and that small-diameter C fibers are preferentially affected at lower doses than larger myelinated fibers.¹ This blockade was found to arise partly from depolarization of the resting membrane potential caused by reduced permeability to potassium and chloride ions, together with suppression of the delayed potassium current that prolongs spike repolarization.1
Central analgesic effects
Beyond interrupting peripheral nerve pain transmission, DMSO exerts direct pain-suppressing effects within the spinal cord and brain:
•Intraperitoneal DMSO (50%) reduced the nociceptive response to capsaicin injection by 73.1% and independently raised pain thresholds in the tail-flick test, with DMSO’s analgesic effect attributed to central (likely NMDA receptor-mediated) mechanisms rather than peripheral afferent modulation.1,2,3
•DMSO microinjected into the rostral ventromedial medulla (a part of the brain) potentiated swim stress-induced analgesia across all phases of the formalin test, likely by increasing neuronal excitability in descending inhibitory pain pathways.1
•In rats, intrathecal DMSO reduced pain transmitting substance P and calcitonin gene-related peptide levels in the spinal cord and increased hot plate latency, indicating direct central antinociception.1 In another study (modeling bone cancer pain) it increased mechanical and thermal pain thresholds and decreased spinal microglial markers (OX-42 and Iba-1), confirming DMSO’s central anti-neuroinflammatory and analgesic properties even in severe pain states.1 Finally, DMSO injected directly into the cerebrospinal fluid has been shown to induce total anesthesia in animals without causing any adverse reactions.1 Additionally, direct application of DMSO into surgical wounds relieved acute pain in rats, providing further evidence of DMSO’s independent analgesic properties at the site of tissue injury.1
•Topical DMSO can also activate spinal inhibitory circuits. Cutaneous application activated Aδ-afferents, which then suppressed C-afferent pain transmission through an intersegmental mechanism mediated by presynaptic GABA(B) receptors on C-afferent central terminals.1
•Additionally, in the spinal nerve ligation (SNL) model of peripheral nerve injury, intrathecal DMSO prevented GABAergic neuron dysfunction and loss in the dorsal horn, central sensitization of dorsal horn neurons, and mechanical hypersensitivity through its free radical scavenging properties.1 This suggests that DMSO may help mitigate central sensitization following certain peripheral nerve injuries.
Dose-dependence
Since DMSO also enhances the function of nerves, in some studies, at low concentrations, it increased rather than reduced pain transmission:
•At very low concentrations (0.3-1%), DMSO enhanced rather than blocked nociceptive transmission in isolated neonatal rat spinal cord, potentiating substance P- and capsaicin-induced depolarization through cholinesterase inhibition (while having no effect on myelinated A-fiber reflexes).1
•In mice, DMSO injected directly into the brain produced strong antinociception (pain reduction), oral administration produced slight antinociception with anti-inflammatory effects, but subcutaneous local administration (which delivers the smallest amount of DMSO to the central nervous system) it increased nociceptive (pain sensing) responses.1
•Cutaneous DMSO enhanced the nociceptive response to capsaicin (a TRPV1 agonist) in a time- and dose-dependent manner: at 30 minutes pre-application, 10-100% DMSO dose-dependently increased the pain reaction, while at 1 minute pre-application (when DMSO had not yet had time to diffuse away to a lower concentration) no effect was seen at any concentration.1
Conversely, low doses of DMSO also have been shown to reduce pain. For example, 0.3% DMSO prevented acetic acid-induced pain behaviors in zebrafish larvae, performing comparably to Tylenol and outperforming ibuprofen (which showed no analgesic effect), likely operating via a Pannexin-1-related pathway.1,2
Note: low concentrations of DMSO masked the antinociceptive activity of Tylenol in the mouse formalin test—however I am not aware of any similar reports in humans.
Lastly, I have not received reports from readers of low doses of topical DMSO worsening pain. However, I am including this section for individuals with challenging pain cases seeking additional insights for developing an effective treatment protocol.
Opioid-independent analgesia and endogenous pain modulation
Opioids work by stimulating pain-blocking receptors that evolved to respond to opioid-like molecules the body naturally produces (endorphins). In 1985, a clinician discovered that giving low doses of an opioid receptor blocker (naltrexone) triggered the body to increase its own endorphin and enkephalin production, and that beyond modulating pain, low-dose naltrexone (LDN) broadly improved immune function, reducing inflammation while increasing resistance to both infections and cancer. As such, LDN (discussed further here) has become an immensely popular integrative therapy (e.g., for fibromyalgia and a variety of autoimmune or chronic inflammatory disorders). Conversely, in opioid users, beyond addiction resulting from the down regulation of the body’s opioid system, a variety of other health issues also emerge such as increased pain sensitivity (opioid-induced hyperalgesia), persistent low mood and anhedonia (loss of ability to enjoy life), hormonal disruptions (such as low testosterone), weakened immune function, reduced bone density, and poorer stress resilience.
DMSO addresses both sides of this equation. As early as 1974, a Nature article noted DMSO held “significant promise for neurological injuries and incapacitating pain” but that it had been “held to an unduly rigorous standard for testing,” leaving it unclear whether its potential would ever be properly studied in humans. Fifty years later, that question remains unanswered, but the evidence for DMSO’s opioid-independent analgesia has only grown stronger.
In direct comparison, DMSO produced analgesic effects comparable in magnitude to morphine, but with a duration of 6–7 hours or sometimes much longer (versus 2 hours for morphine), and this effect was rarely reversed by naloxone, indicating the mechanism is likely independent of opioid receptors.1,2,3,4 Likewise, in horses, IV DMSO produced analgesia clinically similar to phenylbutazone (a potent NSAID), acting via blockade of glutamatergic pathways and NMDA receptors in the CNS rather than through opioid mechanisms, with a half-life of approximately 8.53 hours allowing safe twice-daily administration.1
Beyond providing opioid-independent pain relief, DMSO appears to amplify the body’s own opioid signaling through multiple mechanisms. NMR studies show that enkephalins (the body’s natural opioids) adopt a compact bioactive conformation in DMSO that pre-organizes their key residues into a morphine-like shape capable of activating opioid receptors (potentially enhancing the efficacy of even trace amounts of endogenous enkephalins).1,2 Additionally, in cell culture, 2% DMSO increased functional μ-opioid receptor expression up to 6-fold (while also upregulating κ-opioid receptors) without altering receptor affinity.1 Complementing this, DMSO enables topical opioid delivery. When morphine or enkephalin analogs were dissolved in DMSO and applied topically to mouse tails, they produced potent, dose-dependent analgesia with no detectable systemic absorption, and repeated exposure induced only local (not systemic) tolerance that was blocked by NMDA antagonism.1 This suggests DMSO could enable targeted localized opioid pain relief without the systemic side effects, tolerance, and addiction that make chronic opioid use so problematic.
Together, these findings may suggest DMSO enhances endogenous opioid signaling at both the peptide and receptor level, potentially benefitting chronic opioid users whose endorphin production has been downregulated while also offering some of the benefits of LDN therapy to chronically ill patients.
Note: from the start, DMSO was recognized to potentiate insulin (making diabetics require lower insulin doses to avoid hypoglycemia), and this effect is frequently postulated to result from DMSO’s protein stabilizing qualities making insulin receptors more sensitive to insulin (suggesting it could do the same for opioid receptors). However, while studies show DMSO can promote insulin secretion,1,2 and the disassembly of insulin amyloid fibrils,1,2,3 I have not found any studies showing it improves receptor function (rather, only ones that show in combination with another agent such as resveratrol, ginger, DHC, allicin or DHEA that insulin sensitivity is increased1,2,3,4,5,6,7,8,9 or that at higher concentrations DMSO impairs insulin binding1).
DMSO also directly counteracts the paradoxical pain sensitization that develops with chronic opioid use. In a morphine-induced hyperalgesia model, DMSO inhibited thermal hyperalgesia by reducing spinal dorsal horn TNF-α expression.1,2 A large number of agents dissolved in DMSO have similarly been shown to reverse opioid-induced hyperalgesia, tolerance, and withdrawal across numerous animal models (such as β-elemene⬖ and curcumin⬖), targeting overlapping central pathways including amygdalar glutamatergic signaling, spinal NMDA receptor trafficking, and neuroinflammatory cascades.1,2,3,4,5,6,7,8,9 GSK3 inhibitors SB216763 and SB415286 prevented morphine-induced antinociceptive tolerance and alleviated withdrawal symptoms (grooming, chewing, ptosis) without affecting other withdrawal behaviors.1
Finally, opioids have been recognized to be one of the medications potentiated by DMSO (acute co-administration of 2% DMSO enhanced morphine antinociception1), potentially allowing chronic opioid users to reduce their doses. In instances where the strongest potentiation occurs (IV administration of both concurrently—which occurred during stem cell infusions), there have been reported instances in children and adults of temporary morphine overdose symptoms.1 This opioid-potentiating effect has also been demonstrated clinically: when DMSO was added to intramuscular pethidine in patients with acute pancreatitis, it significantly enhanced pain relief, with 57% of patients pain-free within 12 hours, attributed to DMSO scavenging oxygen-derived free radicals.1
Note: conversely repeated higher doses of DMSO (via microinjections) was found to decrease morphine potency for at least one week (comparably to morphine tolerance).1
In short, research into DMSO’s interactions with opioids, beyond potentially benefitting opioid users, provides additional insights into how DMSO is independently able to improve a variety of chronic pain conditions.
Potentiation of local anesthetics
DMSO significantly enhances the potency of local anesthetics,1,2,3,4 potentiating lidocaine’s nerve conduction blocking effect at concentrations as low as 0.1-0.2% (where DMSO alone has no anesthetic effect), through an allosteric mechanism independent of increased intracellular drug levels.1,2,3,4 In a human study, 50% DMSO alone produced partial anesthesia (numbness) to pinpricking sensation (while 20% produced a smaller reduction),1 and long-term (but fully reversible) blockade of nerve endings and trunks can be achieved by mixing DMSO with local anesthetics at a final concentration of 30-50%.1 In a bilateral CCI (chronic constriction injury) neuropathic pain model, intrathecal procaine dissolved in DMSO significantly improved mechanical and thermal pain thresholds while downregulating JAK2/STAT3 signaling in the spinal dorsal horn, with JAK2 overexpression reversing procaine’s analgesic effect.1
DMSO also markedly enhances transdermal anesthetic penetration (producing higher skin concentrations, greater flux, and shorter lag times compared to other vehicles.1 This penetration-enhancing property led to the early development of tetracaine dissolved in DMSO for topical skin anesthesia,1,2 which did not gain widespread dermal use due to the temporary skin irritation DMSO can cause. However, it found a niche in otology as myringotomies (e.g., for ear tubes) first require the painful injection of an anesthetic into the eardrum (which is avoided with a topical DMSO application), with one paper reporting this combination was well tolerated and effective in 164 cases (with tetracaine inducing anesthesia within 10 minutes).1,2,3
Note: DMSO has also been listed among injectable solutions (alongside lidocaine, procaine, corticosteroids, and B vitamins) for trigger point therapy.1
In one trial, topical DMSO combined with lidocaine provided effective analgesia during extracorporeal shock wave lithotripsy (outperforming EMLA cream with lower pain scores and fewer interruptions from intolerable pain,1 offering a cost-effective alternative to opioids and injectable analgesics while reducing the need for general anesthesia.1 In another, topical lidocaine in DMSO-ethanol safely achieved 51% anesthesia during pulsed dye laser treatment of vascular malformations.1 Likewise, in veterinary practice, topical bupivacaine-DMSO applied to trimmed chicken beaks improved feed intake compared to untreated birds,1
Note: DMSO was anticipated as a dedicated nerve pain drug by Searle, but its development was halted by the FDA.1
Unusual Pain Types
DMSO also treats a variety of pain types that are challenging to treat with conventional options. For example, extensive evidence and numerous reader testimonials1,2,3 show DMSO treats cancer bone metastasis pain.1 Likewise, in 21 patients with acute alcohol-induced pancreatitis rectal DMSO (500 mg every 8 hours) achieved complete pain relief within 12 hours in 57% of patients (vs. 17% controls) and within 24 hours in 100% (vs. 52% controls), enabling hospital discharge after 3 days vs. only 22% of controls by day 5.1,2
Likewise, one author reported DMSO treating challenging phantom limb pain,1 and readers here have as well,1,2,3 including a wheelchair-confined amputee (due to previous strokes and vascular issues) who had a complete resolution of the pain.1 Similarly, DMSO has been consistently observed to treat the severe neuropathic pain quadraplegics frequently experience (which is why Jackson’s mother felt it was so noteworthy he did not need to take any pain medications).
Readers have also reported that DMSO was the only thing that helped other challenging types of pain, such as from polymyalgia,1 horrific gadolinium-induced bone pain,1 or EDS (hypermobility),1,2,3 with one reader sharing DMSO “Gives me a chance to feel what “normal” might be like.”1
Clinical pain data
DMSO has been used clinically for a variety of neuropathic pain conditions, most extensively, as mentioned above for complex regional pain syndrome. Additionally:
•In one study of patients with peripheral neuritis and segmental neuralgia, DMSO gave 66% a full remission and 22% a partial remission.1
•In another study, DMSO was used to treat glossalgia (burning tongue syndrome).1
•DMSO applications are widely recommended across Russian clinical guidelines for neuralgia and neuropathic conditions, where its mechanisms are described as including inactivation of hydroxyl radicals, improvement of metabolic processes at inflammation sites, reduction of excitatory impulse conduction in peripheral neurons, and moderate fibrinolytic activity, while simultaneously enhancing the penetration of analgesic and anti-inflammatory drugs.1,2
Finally, DMSO is generally more effective for treating pain above the waist and is less likely to help larger joints (e.g., the hips, which have the smallest response—although many readers have still reported benefit there). In chronic pain patients who do not respond to topical DMSO, a lower concentration of injectable DMSO or oral DMSO often helps. In some cases, it can take weeks for chronic pain to improve, and it has been noted that for some chronic pain patients, periodic breaks (e.g., 1-2 days a week) are needed to avoid developing a tolerance to DMSO.
Reader Reports (Nerve Pain)
Readers, in turn, report DMSO relieving nerve pain from a wide variety of causes. Several described immediate or near-immediate relief: “Just started DMSO. It’s relieving chronic nerve pain,”1 “It works for me for nerve pain,”1 and a reader with nerve damage from a bad wreck 10 years ago found significant relief.1 One with a pinched nerve and bursitis reported “instant relief,”1,2 while a nurse with a post-surgical pinched nerve from an ankle repair found “pain was gone” overnight after combining DMSO with magnesium.1
Post-Surgical Nerve Damage
Readers with post-surgical nerve damage reported nerve regeneration over time. A reader who lost all feeling in the back of the left arm after a 2003 lumpectomy started using DMSO on the arm: “feeling is returning. Great improvement.”1 Another with nerve damage from ankle surgery hardware found DMSO helpful, and after hardware removal, continued using it for residual nerve effects.1 One reader’s nerve pain from ankle surgery (six years prior) responded the first night of topical DMSO application.1 A reader who had lymph nodes removed under the arm for breast cancer and was left with complete numbness found that after four DMSO applications, feeling returned: “I could not shave my armpit without a mirror as I could not feel anything and last night, shaving with feeling.”1 Another with 15 years of numbness and a persistent weeping wound from a surgical incision found “both issues resolved very quickly” with DMSO.1
Post-Joint-Replacement Nerve Pain
Two readers reported DMSO resolving electrical pins-and-needles sensations at shoulder replacement sites. One applied DMSO along the scar “and the electrical pins and needles sensation has not returned,”1 while another “put it there once and it went away.”1
Burning Pain
A reader’s mother with burning feet “swears by” DMSO for pain relief and has used it for years.1 Another with burning wrist pain found DMSO “mostly taken care of it.”1 An aircraft mechanic with severe neuropathic pain (“like an electrical shock on fire”) in his palm and thumb applied DMSO topically once; the pain resolved and had not recurred over a year later despite continued daily manual work.1
Additional readers reported relief from pinched nerves,1,2,3,4,5,6,7,8,9,10 muscle overuse,1 and neuropathic (nerve) pain of unspecified cause,1,2,3,4,5,6,7,8,10, 11,12,13,14,15,16,17,18,19,20, 21,22,23,24,25,26,27,28,29,30, 31,32,33,34,35,36,37,38,39,40,41 with many noting that nerve pain was particularly responsive to DMSO compared to other types of pain.1,2
Note: one reader with a “mysterious” sensory issue (burning and numbness throughout the body for 9 months, all tests negative) found only temporary improvement from topical 70% DMSO, suggesting that deeper or more systemic neurological conditions may require oral or IV administration.1
Spinal Pain
Nerve pain from a spinal issue (e.g., nerve root compressions and radiculopathies) is highly responsive to DMSO, with hundreds of studies and reader reports attesting to this. This extensive body of evidence is detailed in the previous article (which can be read here).
Combination Studies in Neuropathic Pain Models
A large number of therapeutic agents dissolved in DMSO have demonstrated efficacy across various neuropathic pain models. For example, one study found that DMSO co-administration with the cannabinoid analgesic CT-3 (which alone produced dose-dependent analgesia comparable to morphine without GI ulceration) reduced analgesia while increasing both toxicity and ulceration.
Since DMSO served as the vehicle control in these studies, the agents’ benefits are measured against DMSO’s own baseline analgesic properties, meaning the actual therapeutic gap between treatment and no treatment is likely larger than these studies report. For example, in one study using DMSO as the vehicle for the A3 adenosine receptor agonist IB-MECA, the DMSO vehicle control group showed full reversal of mechanical allodynia in CCI rats, an effect the authors did not comment on but which is consistent with DMSO’s independent analgesic properties.1
Note: one reader cautioned against using DMSO to “transport” CBD cream: “You’ll get hit with a sledgehammer that will make you question life itself.”1This is consistent with DMSO’s known ability to dramatically enhance the absorption and potency of topical agents, and readers should be aware that combining DMSO with other active topical substances (including CBD, essential oils, and capsaicin) may produce effects far stronger than either alone. Conversely, topical WIN 55,212-2 (a cannabinoid agonist) enhanced topical morphine analgesia via CB1 receptor mechanisms,1 and DMSO combined with anandamide⬖ (an endogenous cannabinoid) also effectively reduced pain,1 suggesting cannabinoid-DMSO-opioid combinations can be synergistic when properly dosed.
Common Neuropathic Pain Combinations
Curcumin⬖ is the most extensively studied natural agent for neuropathic pain in combination with DMSO. Across CCI models, intrathecal and intraperitoneal curcumin⬖ repeatedly improved mechanical and thermal pain thresholds through multiple pathways: upregulating cannabinoid receptor 1 while downregulating NMDAR2B, inhibiting the inflammatory TLR4/TNF-α/IL-1β cascade, suppressing TAK1-mediated astrocyte activation, and inhibiting spinal microglial inflammation.1,2,3,4 In spared nerve injury models, curcumin⬖ achieved analgesic effects comparable to pregabalin (likely through reduced CCL2 expression in dorsal root ganglia) and suppressed spinal p38 driven inflammatory cytokine signaling.1,2 With forced exercise, curcumin⬖ prevented peripheral nerve conduction deficits in CCI rats,1 and in diabetic neuropathic pain, attenuated mechanical allodynia with the opioid system implicated in its mechanism.1
Resveratrol⬖ combinations also showed consistent benefits across neuropathic pain models. In CCI rats, intrathecal resveratrol⬖ attenuated thermal hyperalgesia by activating anti-inflammatory SIRT1 and reducing inflammatory acetylated NF-κB, while intracerebroventricular delivery inhibited hippocampal astrocyte activation and NF-κB expression (demonstrating that neuropathic pain involves supraspinal neuroinflammation amenable to treatment).1,2,3 In paclitaxel-induced neuropathy, resveratrol⬖ increased spinal SIRT1 and improved mechanical pain thresholds.1 Sulforaphane⬖ and resveratrol⬖ together produced synergistic analgesia in an orofacial formalin pain model at doses lower than either agent alone required for equivalent effect.1
Numerous p38 MAPK inhibitors reduced neuropathic pain across virtually every model tested, including CCI (reducing P2X7 and P2Y13 receptor expression, suppressing COX-2, and inhibiting microglial inflammation),1,2,3,4 spinal nerve ligation (attenuating allodynia and hyperalgesia both preventively and in established pain),1 ventral rhizotomy,1 diabetic neuropathy (alleviating hyperalgesia and reducing P2X7/TRPV1/PKCε signaling),1,2 and nucleus pulposus-induced radicular pain.1 One, licochalcone A⬖ achieved comparable p38/NF-κB inhibition and microglial suppression in CCI rats.1
CCI (chronic constriction injury) models
Among natural compounds, 1,8-cineole⬖ (the primary component of eucalyptus oil) dose-dependently alleviated neuropathic pain and inhibited P2X3 and P2X2 receptor overexpression in dorsal root ganglia and spinal cord across three studies.1,2,3 Cardamonin⬖ exerted antiallodynic and antihyperalgesic effects (counteracting excessive sensitivity to pain) comparable or superior to amitriptyline through central and peripheral opioidergic system activation.1 Additional natural agents improving pain thresholds in CCI models include astragalin⬖ (which inhibited P2X4/ERK1/2/TNF-R1 signaling and glial activation),1 luteolin⬖ (via the sirt1/FOXO1 pathway),1 carnosic acid⬖ (via Sirt1/p66shc),1 and tetramethylpyrazine⬖ (which dose-dependently inhibited non-L-type calcium currents in dorsal root ganglion neurons).1 Silymarin⬖ produced significant antinociception with a favorable safety profile and low cost.1 Cimifugin⬖ (from Saposhnikovia) reduced formalin-induced flinch responses dose-dependently, with ED50 values of 696 μg for acute pain and 1,243 μg for inflammatory pain.1
CB2 receptor agonists (AM1241) consistently improved mechanical and thermal thresholds in CCI rats across multiple studies, operating through suppression of purinergic receptor signaling (P2X4, P2X7, P2Y12, P2Y13), p38 MAPK/NF-κB pathways, and BDNF, with microRNA-124-3p identified as a mediating mechanism.1,2,3 The synthetic cannabinoid CP55940 similarly dose-dependently suppressed neuropathic pain through CB1 and CB2 receptor activation, inhibiting PKA upregulation, reducing P2X2R and P2X3R expression in dorsal root ganglia, and suppressing intracellular calcium increases in cultured DRG neurons.1,2,3,4
Riluzole attenuated mechanical allodynia and induced long-term depression of C and Aδ fiber-evoked excitatory postsynaptic currents in spinal dorsal horn neurons, while also downregulating P2X7 receptor expression and inhibiting microglial activation through a mechanism distinct from sodium channel blockade.1,2,3 Necrostatin-1 improved mechanical and thermal thresholds by inhibiting the RIP1/RIP3/MLKL necroptosis pathway and reducing IL-1β, TNF-α, and IL-6.1
Additional pharmaceutical agents showing analgesic effects in CCI models include an ERK1/2 inhibitor (U0126, which attenuated neuropathic pain and VEGF/ERK/CREB signaling across multiple studies),1,2,3,4,5 an aquaporin 4 inhibitor (TGN-020, which inhibited ERK/JNK/p38 MAPK signaling),1,2 a Sigma-1 receptor antagonist (BD-1047, which modulated P2X3 receptor co-expression in DRG neurons),1 wortmannin (which alleviated pain via PI3K/Akt/mTOR pathway inhibition and microglial suppression),1 a caspase-1 inhibitor (VX-765, which reduced spinal NLRP1 and IL-1β),1 and a monocarboxylate transporter inhibitor (4-CIN, which completely prevented neuropathic pain development).1 Additional agents reducing pain thresholds through glial or inflammatory suppression include a GSK3β inhibitor and eIF2α agonist (reduced ER stress in DRG),1 a STAT3 inhibitor (WP1066),1 pioglitazone (suppressed astrocyte activation and inflammatory cytokines via PPARγ),1 roscovitine (a CDK5 inhibitor that suppressed astrocyte activation),1 a PKCε inhibitor (BIM I, which reduced astrocyte-mediated central pain sensitization),1 a MIF antagonist (ISO-1, which suppressed TNF-α and IL-1β in DRG),1 a GABA transporter 3 inhibitor (transiently improved pain thresholds by targeting GAT3 upregulation in DRG),1 liproxstatin-1 (mitigated ferroptosis in DRG Schwann cells and astrocytes),1 a HO-1 agonist (cobalt protoporphyrin IX, which increased μ-opioid receptor expression),1 astaxanthin⬖ (elevated HO-1 and antioxidant enzymes while reducing inflammatory cytokines),1 a CB1 agonist (AM841),1 PKA/CaMKII/HCN4 pathway inhibitors,1 dual σ1/μ opioid receptor small molecules,1 a PKC inhibitor (which reduced P2X3R expression),1 and triptolide⬖ (which suppressed T cell activation and spinal inflammation without motor dysfunction).1
SNL (spinal nerve ligation) models
Koumine⬖ (from Gelsemium) dose-dependently reversed mechanical allodynia by acting as a positive allosteric modulator of the translocator protein (TSPO) on spinal astrocytes, stimulating pregnenolone and allopregnanolone production; in a separate study, its analgesic effect was mediated by upregulating spinal 3α-HSD expression, increasing local neurosteroid synthesis.1,2 Sec-O-glucosylhamaudol⬖ (from coastal hog fennel) alleviated mechanical allodynia by inhibiting the p38/JNK MAPK and NF-κB pathways and reducing autophagy, with antinociceptive effects reversed by naloxone (indicating μ-opioid receptor involvement).1,2 Tetrahydropalmatine⬖ significantly increased mechanical and thermal pain thresholds at medium and high doses.1
Rapamycin was the most extensively studied pharmaceutical agent in SNL models, consistently improving pain thresholds across five studies by enhancing spinal autophagy (increasing LC3-II and Beclin-1, decreasing p62), reducing neuronal apoptosis (decreasing caspase-3, increasing NeuN), and suppressing astrocyte activation (reducing GFAP). At the molecular level, rapamycin reduced mTOR/NR2B signaling, and autophagy activation reduced spinal IL-1β, TNF-α, and reactive oxygen species via the JNK/NF-κB pathway, with NRF2 partially mediating autophagy’s regulation of ROS. Conversely, the autophagy inhibitor 3-MA worsened pain behaviors and increased neuronal apoptosis.1,2,3,4,5
Trichostatin A (TSA) and other HDAC inhibitors repeatedly attenuated mechanical allodynia in SNL and related models by reversing differential miRNA expression, upregulating BDNF, and modulating histone acetylation in the spinal cord.1,2,3 Additional agents demonstrating efficacy in SNL models include a KDM6B inhibitor (GSK-J4, which epigenetically regulated IL-6 via H3K27me3 demethylation and STAT3 signaling),1 a BRD4 inhibitor (I-BET762, which identified the miR-200a/c-myc/ROS axis as a regulatory mechanism),1 a P2Y12 receptor antagonist (MRS2395, which suppressed P2X4 and p38 MAPK),1 meloxicam (which prevented allodynia development when administered early after injury, supporting a role for COX-2 in neuropathic pain pathogenesis),1 and an AKT inhibitor (which enhanced autophagy and provided analgesic effects by modulating the AKT/TSC2/mTOR pathway).1 In bone cancer pain models, aspirin-triggered lipoxin significantly increased paw withdrawal threshold with analgesic duration exceeding equimolar morphine,1 while baicalein⬖ (attenuated mechanical allodynia; both reduced 5-lipoxygenase and p-JNK in the spinal cord).1
Note: garcinol (a p300 acetyltransferase inhibitor) reduced thermal hyperalgesia and suppressed NF-κB pathway activation via reduced p300-mediated acetylation of p65 in SNL rats.1,2 A TRPM8 blocker (AMTB) reversed both cold hyperalgesia and mechanical hyperalgesia in SNI rats while simultaneously restoring scratching behavior suppressed by nerve injury, revealing that neuropathic pain and itch share overlapping spinal mechanisms.1 Among agents combined with DMSO for spinal nerve injury models, a TSPO agonist (Ro5-4864) reduced spinal astrocyte activation (GFAP) and TNF-α for up to 21 days after nerve injury,1 tetramethylpyrazine⬖ inhibited non-L-type calcium currents in dorsal root ganglion neurons,1 a p38 MAPK inhibitor reduced spinal p-p38 and serum IL-6 while upregulating glucocorticoid receptors,1 and rufinamide selectively suppressed C-fiber (but not Aδ-fiber) excitatory transmission in spinal substantia gelatinosa neurons.1
SNI (spared nerve injury) models
In addition to the curcumin⬖ and p38 inhibitor studies described above, agents improving pain thresholds in SNI models include protectin D1 (which dose-dependently increased paw withdrawal threshold via PPARγ activation while reducing TNF-α and IL-6),1 bardoxolone methyl (an Nrf2 activator),1 memantine (which dose-dependently attenuated mechanical hyperalgesia and allodynia via NMDA open-channel blockade at clinically tolerable doses without motor deficits often seen with this medication class),1 and intrathecal modulators of nNOS phosphorylation sites (identifying CaMKII and Akt as key regulators of nitric oxide-mediated neuropathic pain).1 A D2 receptor antagonist (sulpiride) partially reversed tramadol’s analgesic effect in CCI rats, demonstrating that tramadol’s pain relief operates partly through dopamine D2 receptor upregulation in the nucleus accumbens.1 A calpain inhibitor reduced mechanical hyperalgesia in a postoperative pain model by reversing KCC2 downregulation in the spinal cord.1
Diabetic neuropathic pain
Among natural compounds, berberine⬖ dose-dependently reduced blood glucose, alleviated mechanical and thermal hyperalgesia, reduced spinal cord and DRG oxidative stress and inflammation, and upregulated μ-opioid receptor expression.1 Osthole⬖ improved pain thresholds while reducing P2X4 receptor expression, GFAP, BDNF, and p38 MAPK phosphorylation in DRG.1 Additional agents include Urtica dioica⬖ and pioglitazone (each improved oxidative stress markers and mitochondrial function while reducing pain scores),1 a TrkB inhibitor (k252a, which significantly increased pain thresholds by decreasing BDNF and increasing KCC2 expression),1 and PI3K/AKT/mTOR pathway inhibition (which promoted spinal autophagy and improved hyperalgesia thresholds).1 Calcitriol (vitamin D)⬖ significantly increased pain tolerance in both tail flick and hot plate tests at 30 and 60 minutes.1 Lastly, alpha-lipoic acid⬖ significantly corrected established hypoalgesia (lost sensation) after 90 minutes, suggesting that once hypoalgesia develops, different therapeutic approaches are needed.1
Chemotherapy-induced neuropathy
Among natural compounds, glucoraphanin⬖ and sulforaphane⬖ dose-dependently reduced oxaliplatin-induced neuropathic pain through H₂S release and Kv7 potassium channel modulation, with daily administration preventing neuropathy development entirely.1 Tanshinone IIA,⬖ cryptotanshinone⬖, and Danshen extract⬖ from Salvia miltiorrhiza alleviated oxaliplatin-induced neuropathic pain while showing selective neuroprotective effects (inhibiting glioblastoma cells with no effect on healthy cells).1 Paeoniflorin,⬖ attenuated paclitaxel-induced mechanical allodynia and demyelination via adenosine A1 receptor activation while downregulating ER stress in Schwann cells.1 Gastrodin⬖ combined with vincristine not only improved tumor inhibition rates but also dose-dependently inhibited vincristine-induced neuropathic pain by suppressing the Notch/CX3CR1/p38 pathway.1 4-Dimethylamino chalcone inhibited myeloperoxidase activity, produced acute antinociception via muscarinic and opioid receptors, and prevented proinflammatory macrophage polarization in vincristine-induced peripheral neuropathy.1 Systemic cannabidiol⬖ (CBD) produced antinociceptive effects in CCI neuropathic pain through peripheral μ- and δ-opioid receptor activation, with the aminopeptidase inhibitor bestatin potentiating CBD’s analgesic effects at lower doses.1 CB2 receptor agonists in DMSO dose-dependently suppressed established paclitaxel-induced mechanical allodynia, normalizing thresholds to pre-paclitaxel baseline.1
Other pain models
Intrathecal cannabinoid receptor agonists (anandamide⬖ and WIN 55,212-2) suppressed allodynia and spontaneous pain attacks in rats with central pain syndrome, with WIN 55,212-2 producing more pronounced and longer-lasting analgesia (80% arrest rate) while high-dose intravenous anandamide⬖ mitigated visceral nociception through CB1 receptor activation in sensitized rats.1,2 Dexmedetomidine attenuated remifentanil-induced hyperalgesia by downregulating NR1 and NR2B subunit expression and membrane trafficking while reducing PKCγ and CaMKIIα phosphorylation in the spinal cord.1 CDDO (a synthetic triterpenoid) exerted analgesic and neuroprotective effects in a postherpetic neuralgia model by reducing TRPV1-positive nociceptive neurons, decreasing neuronal apoptosis, reversing glial cell activation (including the first reported role of oligodendrocytes in postherpetic neuralgia), and suppressing PKC-δ and phosphorylated Akt signaling.1 Sesamin⬖ reduced both acute and chronic formalin-induced pain while downregulating TLR4/NF-κB/NLRP3 inflammatory signaling in brain tissue.1 Intraperitoneal nifedipine dissolved in DMSO produced significant dose-dependent antinociception (5-15 mg/kg) in rats, with a positive dose-response correlation suggesting involvement of spinal calcium channel mechanisms.1
Among agents studied in bone cancer pain models, resveratrol⬖ increased pain thresholds and modulated OPG/RANK/RANKL while decreasing TNF-α, IL-6, IL-1β, and CCL2,1 koumine⬖ decreased spinal GFAP, Iba-1, IL-6, IL-1β, and TNF-α,1 tanshinone IIA⬖ reduced spinal IL-1β, IL-6, and TNF-α,1 curcumin⬖ elevated mechanical withdrawal threshold and reduced spinal p-CaMKII,1 and the CB2 agonist JWH015 relieved both mechanical and thermal hyperalgesia with CB2 receptor expression upregulating over time.1
Lastly, a Russian “Espol” ointment containing DMSO combined with capsicum extract⬖ and coriander essential oil⬖ was formulated for neuralgias, radiculitis, myositis, and bruises, providing hyperemia alongside analgesic and anti-inflammatory effects.1 A veterinary remedy for pain in arthritis, arthrosis, and neuralgia in dogs was formulated with DMSO, menovasin (containing menthol, procaine, and benzocaine), May honey, egg yolk, and ghee butter.1
Fibromyalgia
A Russian study on primary fibromyalgia syndrome found that combined therapy using DMSO with non-hormonal anti-inflammatory agents and acupuncture sessions promoted normalization of dysfunctions and was noted as “easy-to-use, available, and inexpensive.”
Over the years, numerous cases of individuals with fibromyalgia having massive improvements in quality of life from DMSO have been reported, but simultaneously, quite a few cases have required starting slowly for sensitive patients with pre-existing toxicity (as otherwise the initial fluid mobilization within their body was too much for the individual—which synopsizes two of the three significant adverse reactions to DMSO I’ve seen within the roughly 10,000 reader reports I’ve reviewed).
While no formal studies have been published beyond the Russian one, Stanley Jacob (whom I consider to be extremely honest) attested:
“Over the last few years, we have been treating patients with fibromyalgia. Seventy percent of the patients have experienced benefit. No serious side effects have been encountered. The properties of our regime contributing to benefit included free-radical scavenging, analgesia, anti-inflammation, softening of scar tissue, reduction of muscle spasm, and stimulation of healing.”
Note: Jacob’s student later published one particularly profound fibromyalgia improvement.1
Readers, in turn, have reported DMSO’s life-changing utility for fibromyalgia. One reader, pain-free for the first time in 25 years, wrote: “I sought out DMSO and it has completely eliminated all of my pain. For reference, I’m a fibromyalgia chronic pain sufferer, in early stages of rheumatoid arthritis, with a connective tissue disorder.”1 Numerous readers credited DMSO with eliminating or greatly reducing longstanding fibromyalgia pain,1,2,3,4,5,6,7,8,9,10,11,12,13 with one’s mother “shocked at how quickly the pain lessened” from the 70% gel.1
Several readers noted the importance of starting slowly with fibromyalgia. One experienced three days of feeling better followed by a return to baseline, a pattern they had seen with many treatments,1 while another found that a three-day oral course (a small teaspoon daily) reduced pain by about 25% and made other pain protocols more effective, with no subsequent loss of efficacy.1
A reader with fibromyalgia for 16 years who had been on gabapentin (which stopped working) and could not get Lyrica from the VA described remarkable results: pain in the left shoulder and blade, cervical and low back pain, knee arthritis, hip pain, scoliosis, neuropathy in both feet, and asthma all improved with topical DMSO, allowing discontinuation of multiple medications including inhalers.1 Another reader used DMSO topically and orally and “had no fibromyalgia or pain for almost 5 years.”1
Headaches & Migraines
Headaches are among the most common and challenging neurological complaints, and one of the conditions for which DMSO was first recognized as effective. Tension headaches (arising from muscular tension in the neck and scalp) and sinus headaches tend to respond well to DMSO, whereas migraine and cluster headaches are less consistently responsive, although some mechanistic evidence has now emerged supporting DMSO’s use in migraines.
Clinical Evidence
DMSO’s use for headaches has been documented since the mid-1960s. A 1985 survey of DMSO users found headaches among the most commonly self-treated conditions, and papers from the early 1980s noted that DMSO was used for headaches among its many applications and a 2005 paper reported that migraine improvements had been attributed to DMSO.1,2,3
The most comprehensive clinical data comes from Stanley Jacob, who reported on 59 patients with headaches from a variety of causes, of whom over 75% responded to topical DMSO. This included 13 out of 17 patients with chronic cervical arthritis-triggered headaches (who then required gradually decreasing doses), 4 out of 5 patients with sinus headaches, both patients with temporal arteritis (complete recovery), and 26 out of 35 patients with trigeminal neuralgia of more than a year’s duration (13 achieving full recovery).
Note: one anecdotal report describes a splitting headache resolving within minutes of DMSO application by Dr. Jacob, returning after four hours, and then leaving permanently after a second application.
In a study where DMSO was found (via electromyography) to relax cervical musculature within 60 minutes of topical application, this relaxation also alleviated associated tension headaches.1,2 Their combined results were as follows:
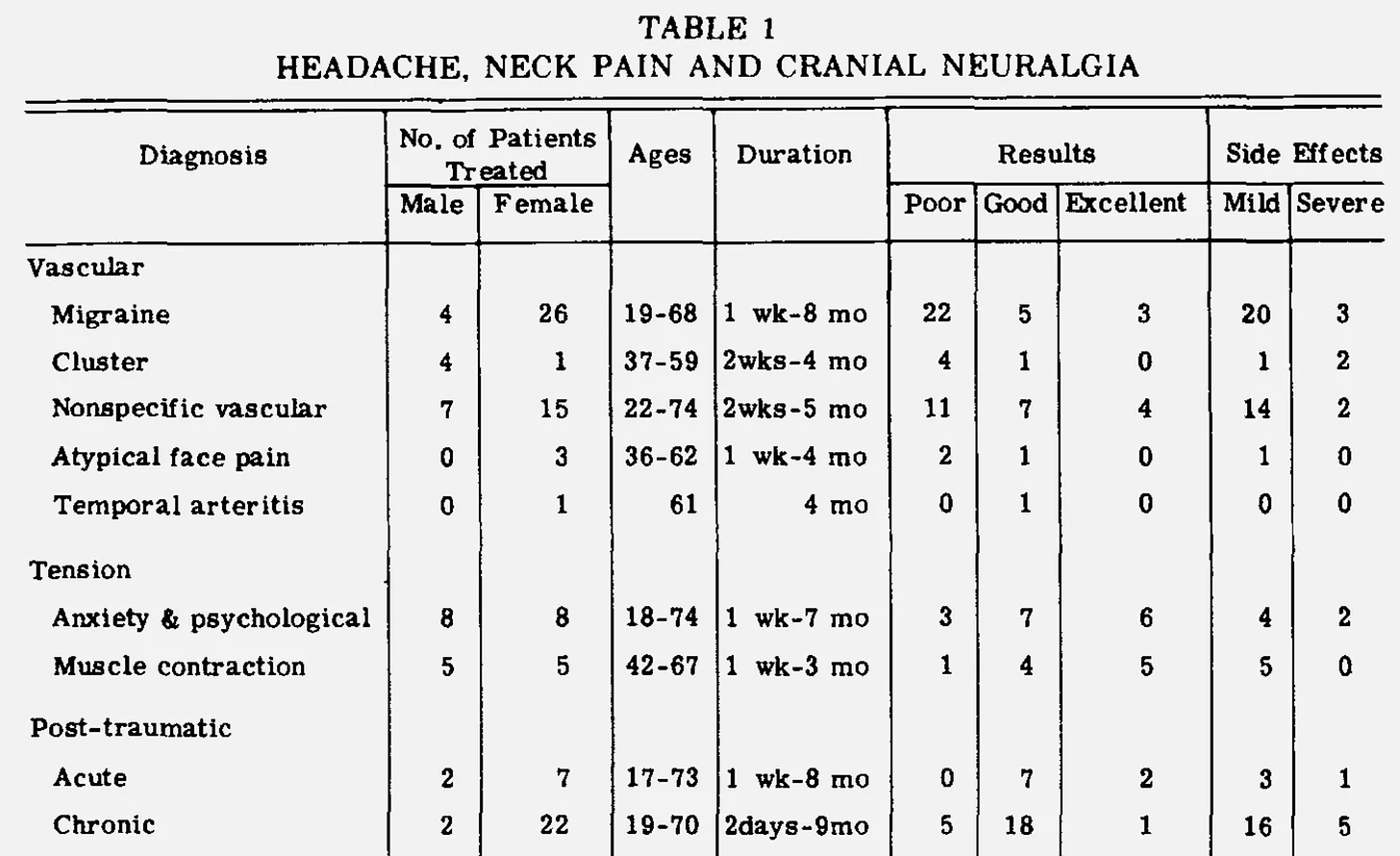
Another study of 10 patients with headaches from various causes (primarily frontal) found DMSO significantly helped all 10, including those who had had headaches for more than a day, with relief times ranging from 1 minute to about 3 hours.1,2 In a study of 15 patients with tinnitus who had concurrent headaches, DMSO produced complete headache recovery in 7, less intense headaches in 1, only occasional headaches in 2, and no response in 1.
In a larger observational series of 190 patients (286 conditions), topical 90% DMSO for headache and neck pain produced poor results in 59, good in 60, and excellent in 35, with better responses in tension, post-traumatic, cervical disc, and sinusitis-related cases, while vascular headaches (migraine, cluster) generally responded poorly.
For sinus-associated headaches, 0.5 ml of 50% DMSO instilled into each nostril was found effective. In children with headaches and cervical spine disorders (105 patients aged 5-18), DMSO applications mixed with novocaine and ATP were recommended when cervicalgia was complicated by myotonic and neurodystrophic syndromes, with 10-15 applications as part of adjunctive therapy.
Lastly, it is important to remember DMSO’s headache reducing qualities often reflect it shifting systemic issues within the body. For example, a case report of a 38-year-old woman with refractory systemic lupus erythematosus documented that topical DMSO resolved severe headaches alongside dramatic improvement in skin lesions and other lupus manifestations, with sustained remission after tapering prednisone.
Migraine Mechanisms
While DMSO’s clinical effects on migraines have been inconsistent, research on cortical spreading depression (CSD, the electrophysiological wave underlying migraine aura) has revealed that DMSO directly modulates the hemodynamic events thought to drive migraine headache.
In rats, 10% DMSO applied to the brain interrupted the dilating vascular changes caused by CSD, likely preventing or attenuating migraine attacks. A more detailed study using laser speckle and optical intrinsic signal imaging found that topical DMSO (0.1-4%) increased resting pial arteriolar diameter and blood velocity in a dose-dependent manner while attenuating the additional hyperemic surge that accompanies CSD. The core CSD wave itself was unaffected; DMSO appeared to stabilize baseline cerebral perfusion, leaving less capacity for the exaggerated vascular overshoot thought to contribute to headache development.1,2 Separately, daily intraperitoneal lamotrigine in DMSO suppressed rat CSD frequency by 37-60% (depending on brain region) over four weeks, outperforming valproate and riboflavin given in saline.
In a clinical study of 120 patients with combined migraine and cervicogenic headache, comprehensive cervical treatment including 10 topical applications of DMSO mixed with novocaine reduced migraine attack frequency by up to 50%, decreased pain intensity, and improved quality of life. An accompanying in vitro experiment using isolated rat skulls demonstrated that DMSO at 1% and 10% dose-dependently increased action potential frequency in trigeminal afferents followed by desensitization (similar to capsaicin), providing a mechanistic explanation for DMSO’s analgesic action in blocking trigeminal pain conduction relevant to headache pathogenesis.1,2,3
Note: I believe blood stasis (which DMSO addresses) plays a key role in migraines.
Reader Headache Reports
Readers consistently reported rapid headache relief from topical DMSO (with a variety of application developed depending on the type of headache1,2,3 such as those from an acute viral illness1). Many readers described headache relief, often within minutes using DMSO,1,2,3 (e.g., “DMSO is the only thing that stops my headaches in their tracks.”1). A reader with chronic headaches for two years following carbon monoxide exposure found DMSO “ended the headaches within two months” when doctors had nothing for the condition.1 Multiple readers described DMSO replacing their regular use of aspirin, NSAIDs, or other headache medications.1,2
Notably, a physician reader applied DMSO to a physician colleague with intractable headaches that “none of the neurologists could fix,” resulting in a complete cure with no further treatment needed; their colleague had been considering quitting work because of the headaches.1
Additional readers reporting (often immense) headache relief include those using DMSO for sinus headaches,1,2 cluster headaches,1 tension headaches,1,2 post-concussion headaches,1 and general chronic headaches.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20
Note: one reader experimented with subcutaneous DMSO injections (6.25% concentration) and reported that injection near the trapezoid produced “horrible headache the day after the injection, then a week of headache free,” suggesting a neural therapy-like reset mechanism.1
Migraines Reports
Migraine responses were more variable but included striking successes. One reader who had lived with chronic migraines since age 7 found that DMSO drops at the onset of aura caused the “aura disappeared and dissolved. No pain within a half hour. I don’t leave home without it now. Changed my life.”1 A reader’s husband with migraines 2–3 times weekly for 30 years has had only one in 45 days since starting DMSO.1 Another couple reported that for the wife’s 30+ years of daily migraines, DMSO “at least has an effect,” and “for the first time in many, many years I heard her say, my head is not hurting.”1 while another reported “I’ve suffered my whole life and this is the first thing to take it away.”1 A reader’s daughter with a migraine applied the DMSO roll-on to her forehead: “Minutes later she was literally snoring and woke up in the morning pain free.”1
Multiple readers noted that catching the migraine early was essential for DMSO to work,1,2,3 consistent with the clinical observation that migraines respond best to DMSO in the early stages.
Many other readers also reported migraine relief.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19 However, a few readers noted that DMSO at higher oral doses triggered headaches or migraines in them,1,2,3 with one identifying a clear dose-response relationship and suspecting interaction with chronic sinus inflammation.1 This is consistent with the biphasic dose response observed in the research literature.
Note: many headaches are incorrectly categorized as migraines.
A New Relationship With Pain
In our society, pain is typically viewed as something to be feared and suppressed. However, I’ve long believed it should instead be seen as a necessary warning, since in many cases it serves as an overt or subtle indicator that something is wrong and an opportunity exists to improve your health.
In this article, I’ve tried to touch upon the deep relationship between the health of the nervous system and the pain we experience, and to show that by healing nerves through giving them what they need, you can frequently eliminate pain rather than having to continually suppress it.
Likewise, even in cases where full resolution is not possible, DMSO offers a way to dramatically improve these debilitating conditions and give patients a life that is not defined by pain or by the toxic medications they wish they could stop taking. I try very hard throughout these articles to avoid sensationalizing and to instead present the information in a balanced and objective way, but I must emphasize here that the suffering chronic pain patients experience is immense, to the point that many eventually take their own lives, and it is simply unconscionable that solutions like DMSO have been suppressed for over fifty years to protect the pain management industry.
In the final part of this article, I will provide practical guidance on sourcing DMSO and detailed dosing protocols for each route of use (including intravenous), so that you and your doctor have the tools to use DMSO for the ailments you encounter. Additionally, I will cover:
- Condition-specific treatment protocols for the conditions discussed throughout this article, such as the pain conditions covered here (e.g., headaches and migraines, trigeminal and post-herpetic neuralgia, and other forms of neuropathic pain) and the numerous neuropathies (including nerve palsies and compression neuropathies like carpal tunnel syndrome and sciatica), along with non-DMSO approaches that help these conditions.
- Protocols for the central nervous system conditions covered earlier in this series (e.g., strokes, Alzheimer’s, Parkinson’s, fatigue, brain fog, chronic stress, cognitive impairment, and developmental delay) and a wide range of spinal conditions (e.g., back or neck pain, disc issues, radiculopathies, and spinal cord injuries).
- Scar treatment and resources for individuals interested in obtaining neural therapy.
- The specific agents that can be combined with DMSO to enhance its efficacy in the conditions detailed throughout this article (e.g., beyond how DMSO is applied for neuropathic pain affecting how well it works, a few agents have proven remarkably effective in combination with DMSO for it).

Your Tax Free Donations Are Appreciated and Help Fund our Volunteer Website
Disclaimer: We at Prepare for Change (PFC) bring you information that is not offered by the mainstream news, and therefore may seem controversial. The opinions, views, statements, and/or information we present are not necessarily promoted, endorsed, espoused, or agreed to by Prepare for Change, its leadership Council, members, those who work with PFC, or those who read its content. However, they are hopefully provocative. Please use discernment! Use logical thinking, your own intuition and your own connection with Source, Spirit and Natural Laws to help you determine what is true and what is not. By sharing information and seeding dialogue, it is our goal to raise consciousness and awareness of higher truths to free us from enslavement of the matrix in this material realm.
























{kind=link}