 EN
EN FR
FR
The prevailing narrative tells us that vaccinating the frail and elderly against Covid had a dramatic effect on mortality. How strong is the presumed effect of a Covid vaccine in that vulnerable population? Is it as strong as many believe, or perhaps much closer to zero than to the other end of the scale?
First, there is bad news to share, even before estimating any possible benefit.
Data from Denmark, Israel, and Sweden show increased risk of infection within one week or so after the first dose. Possible mechanisms include transient immunosuppression (decreased lymphocyte count), conversion of asymptomatic infection to symptomatic infection, and infection at vaccination sites. News outlets in Israel reported outbreaks of Covid infections in nursing homes shortly after the initiation of the vaccination campaign, and again after initiating the booster campaign (use Google Translate). Needless to say, when the risk of infection increases, the risk of death increases too.
Skipping the hazard period, studies of vaccine effectiveness (thereafter, VE) reported a remarkable result that should have surprised knowledgeable readers. Estimates for the elderly have been extremely high, sometimes similar to those for younger age groups. For instance, a study in Israel of elderly residents of long-term care facilities reported VE of 85 percent against Covid death.
That is not only contrary to basic knowledge from immunology but is also incompatible with the following observation:
“After the second vaccination [by the Pfizer vaccine] 31.3% of the elderly [over the age of 80] had no detectable neutralizing antibodies in contrast to the younger group, in which only 2.2% had no detectable neutralizing antibodies.” (My italics)
Consider three facts:
- Almost one-third of the elderly (over the age of 80) do not develop antibodies after vaccination against Covid
- Vaccine-induced immune response is known to attenuate with aging
- Flu vaccines do not offer high protection in the elderly
How could Covid vaccines have been highly effective in the frail and elderly?
They were not. VE values that are much higher than 50 percent are a priori implausible. Anecdotally, that’s an estimate from a simple comparison of vaccinated and unvaccinated residents of nursing homes in Sweden. Likewise, the aforementioned study in Israel (overall VE of 85 percent) indeed noted that effectiveness decreased as age increased. VE by age group was not reported.
But even 50 percent might be overly optimistic.
Several sources of bias have affected observational studies of Covid vaccines. I will focus on one which I think ranks high on the list. Most important, it can be roughly accounted for.
A naïve comparison of vaccinated people with unvaccinated people is grossly misleading because of the “healthy vaccinee” bias, demonstrated repeatedly and better explained in the reverse direction. People who are not vaccinated are, on average, less healthy than their vaccinated counterparts, and therefore have higher mortality in general. The mechanisms behind this phenomenon deserve a separate discussion, but it is well documented, nonetheless. Previous research on flu vaccines has also shown that the bias is not easily removed by conventional statistical methods.
Which means that even if nursing home residents in Sweden, in Israel, or elsewhere were unknowingly injected with placebo, instead of a vaccine, Covid mortality would have been higher in non-injected residents. We would have computed biased (false) VE, attributed to placebo.
How strong is the bias? What is the typical “general mortality” ratio, comparing unvaccinated to vaccinated in the population? If we know the ratio — the bias factor — we can replace biased estimates of VE with at least roughly corrected estimates. That’s better than no correction at all.
Fortunately, we have estimates of that ratio from studies that compared non-Covid mortality in the two groups. Since Covid vaccines are not expected to reduce non-Covid mortality, any ratio higher than 1 is an estimate of the bias factor. (To simplify, I ignore the influence of vaccine-related death on that ratio.)
Based on data from the US and the UK, the lower bound of the bias factor is about 1.5, and the likely value is somewhere between 2 and 3: In general, the mortality rate of unvaccinated is 2 to 3 times the mortality rate of vaccinated. Some variation by age and other factors is expected.
I show here one example (Table) from a large cohort study in the US (where the unvaccinated group was “diluted” by those who were vaccinated later).
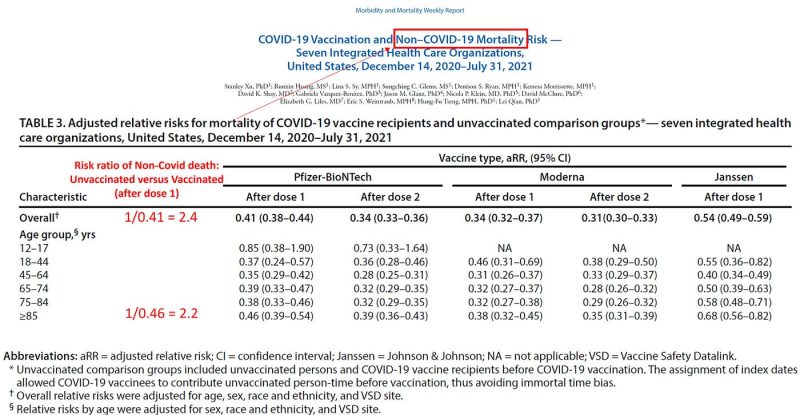
The relative risks (or risk ratios) of non-Covid death demonstrate the healthy vaccinee bias. They are all below 1, indicating that those who were vaccinated against Covid were less likely to die — from non-Covid causes! — than their unvaccinated counterparts. The inverse of these numbers is the bias factor, which ranges between 2 and 3, overall and in most age groups including the oldest (2.2).
Once the bias factor is estimated, say 2, correction of biased VE is simple.
Consider, for example, that biased VE of about 50 percent from Sweden, which was based on a comparison of vaccinated and unvaccinated residents of nursing homes. VE of 50 percent is derived from a (biased) risk ratio of 0.5: vaccinated appear to be at half the risk of Covid death, or vice versa: unvaccinated appear to have twice the risk of Covid death (supposedly because they were not vaccinated). Since the latter have twice the risk of death to begin with, vaccination has made no difference. Multiplying the biased risk ratio (0.5) by the bias factor (2) restores the null effect (risk ratio = 1) and the correct VE (0 percent).
If the bias factor was only 1.5, that biased VE of 50 percent from Sweden will be corrected to 25 percent, much closer to futile than to a highly effective vaccine.
The correction method is approximate, and the healthy vaccinee bias is not the only culprit. What VE would we have observed had we been able to remove other biases as well?
We have to struggle with complicated biases in observational studies because we don’t have randomized trials with a mortality endpoint. And that is nothing short of scandalous. Let me end by explaining why it is scandalous and why there are no data.
When randomized trials were initiated, the pandemic might have been called “the nursing home pandemic” because 30 to 60 percent of Covid deaths occurred in nursing homes. Sweden was a prime example.
With that in mind, any first-year student in epidemiology will tell you that the first placebo-controlled randomized trial of a Covid vaccine should have been conducted in nursing homes, relying on “hard endpoints” — hospitalization and death. Not only should we establish benefits in the most afflicted population, but such a trial would have been statistically efficient, given the expected mortality rate. It would also have been highly feasible in terms of recruitment and follow-up. Having no meaningful mortality data from a randomized trial of a Covid vaccine is scandalous indeed. Who should be held accountable?
No such trial was initiated because the big money was going to follow mass vaccination. Therefore, the pharmaceutical industry, with silent agreement of public health officials, focused on symptomatic infection as an endpoint — rather than death — in younger and healthier populations. Moreover, knowing the attenuated immune response in the elderly, they likely feared that studies of the mortality endpoint in nursing home residents would not deliver stellar results. And even if favorable, the results might not have sufficed for authorizing mass vaccination.
To the list of public health misfeasance during the pandemic, we should add at least one nonfeasance: failure to demand randomized trials of vaccine effectiveness in nursing home residents. I suspect that if such trials were conducted early on, google search of “vaccine mandate” would not have returned 100 million results.
From brownstone.org

Your Tax Free Donations Are Appreciated and Help Fund our Volunteer Website
Disclaimer: We at Prepare for Change (PFC) bring you information that is not offered by the mainstream news, and therefore may seem controversial. The opinions, views, statements, and/or information we present are not necessarily promoted, endorsed, espoused, or agreed to by Prepare for Change, its leadership Council, members, those who work with PFC, or those who read its content. However, they are hopefully provocative. Please use discernment! Use logical thinking, your own intuition and your own connection with Source, Spirit and Natural Laws to help you determine what is true and what is not. By sharing information and seeding dialogue, it is our goal to raise consciousness and awareness of higher truths to free us from enslavement of the matrix in this material realm.
























{kind=link}
I feel sick to the pit of my stomach and my heart hurts to think that the vulnerable and the innocent have been maimed and murdered and despite the level of evidence against these criminals they are still being allowed to carry on doing just what they like because they have infiltrated every department where power is.