Bernhard Metzler, Peter Siostrzonek, Ronald K Binder, Axel Bauer, Sebastian Johannes Reinstadler.European Heart Journal, April 16
We conducted a nationwide retrospective survey on the impact of COVID-19 on the diagnosis and treatment of acute cornary syndrome (ACS) from 2 to 29 March in Austria.
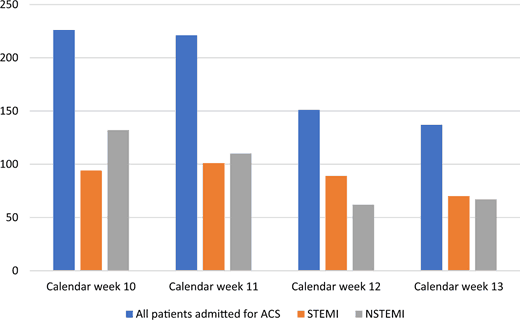
Of the 19 public primary percutaneous coronary (PCI) centres contacted, 17 (90%) provided the number of admitted patients.During the study period, we observed a significant decline in the number of patients admitted to hospital due to ACS (Figure1).Comparing the first and last calendar week, there was a relative reduction of 39.4% in admissions for ACS.In detail, from calendar week 10 to calendar week 13, the number of ST-segment elevation myocardial infarction (STEMI) patients admitted to all hospitals was 94, 101, 89, and 70, respectively.The number of non-STEMI patients declined even more markedly from 132 to 110, to 62, and to 67.
Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19.The absolute numbers of all ACS (blue bars), STEMI (orange bars), and NSTEMI (grey bars) admissions in Austria from calendar week 10 to calendar week 13 are shown.Abbreviations: STEMI, ST-segment elevation myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction.
Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19.The absolute numbers of all ACS (blue bars), STEMI (orange bars), and NSTEMI (grey bars) admissions in Austria from calendar week 10 to calendar week 13 are shown.Abbreviations: STEMI, ST-segment elevation myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction.
The main finding of our retrospective observational study is an unexpected major decline in hospital admissions and thus treatment for all subtypes of ACS with the beginning ofthe COVID-19 outbreak in Austria and subsequentlarge-scale public health measures such as social distancing, self-isolation, and quarantining.
Several factors might explain this important observation.The rigorous public health measures, which are undoubtedly critical for controlling the COVID-19 pandemic, may unintentionally affect established integrated care systems. Amongst others,patient-related factors could mean that infarct-related symptoms such as chest discomfort and dyspnoea could be misinterpreted as being related to an acute respiratory infection.
Moreover,the strict instructions to stay at home as well as the fear of infection in a medical facility may have further prevented patients with an ACS from going to a hospital.
Irrespective of the causes, the lower rate of admitted and therefore treated patients with ACS is worrisome and we are concerned that this might be accompanied by a substantial increase in early and late infarct-related morbidity and mortality.
Our study does not provide data on mortality; however, considering the annual incidence of ACS in Austria (200/100 000/year = 17 600/year in 8.8 million habitants)1and taking into consideration sudden cardiac deaths and silent infarctions (one-third), there will remain ∼1000 ACS cases a month.The difference between the assumed number of ACS patients and the observed number in our study, i.e. 725 ACS patients in calendar weeks 10–13 is 275.According to these assumptions, 275 patients were not treated in March 2020.
Based on data showing that the cardiovascular mortality of untreated ACS patients might be as high as 40%(as it was in the 1950s),2we can theoretically estimate 110 ACS deaths during this time frame.The number of deaths associated with this unintentional undersupply of guideline-directed ACS management is very alarming, particularly when considering thatthe official number of COVID-related deaths in Austria was 86 on 29 March.
In conclusion, it seems likely that the COVID-19 outbreak is associated with a significantly lower rate of hospital admissions and thus, albeit unintended, treatment of ACS patients,which is most likely explained by several patient- and system-related factors.Every effort should be undertaken by the cardiology community to minimize the possible cardiac collateral damage caused by COVID-19.
References
1 Widimsky P, Wijns W, Fajadet J, de Belder M, Knot J, Aaberge L, Andrikopoulos G, Baz JA, Betriu A, Claeys M, Danchin N, Djambazov S, Erne P, Hartikainen J, Huber K, Kala P, Klinceva M, Kristensen SD, Ludman P, Ferre JM, Merkely B, Milicic D, Morais J, Noc M, Opolski G, Ostojic M, Radovanovic D, De Servi S, Stenestrand U, Studencan M, Tubaro M, Vasiljevic Z, Weidinger F, Witkowski A, Zeymer U; European Association for Percutaneous Cardiovascular Interventions.Reperfusion therapy for ST elevation acute myocardial infarction in Europe: description of the current situation in 30 coutries.Eur Heart J 2010;31:943–957.
2 Luscher T, Obeid S.From Eisenhower’s heart attack to modern management: a true success story!Eur Heart J 2017;38:3066–3069.
Your Tax Free Donations Are Appreciated and Help Fund our Volunteer Website
Disclaimer: We at Prepare for Change (PFC) bring you information that is not offered by the mainstream news, and therefore may seem controversial. The opinions, views, statements, and/or information we present are not necessarily promoted, endorsed, espoused, or agreed to by Prepare for Change, its leadership Council, members, those who work with PFC, or those who read its content. However, they are hopefully provocative. Please use discernment! Use logical
thinking, your own intuition and your own connection with Source, Spirit and Natural Laws to help you determine what is true and what is not. By sharing information and seeding dialogue, it is our goal to raise consciousness and awareness of higher truths to free us from enslavement of the matrix in this material realm.
Cookies
To make this site work properly, we sometimes place small data files called cookies on your device. Most big websites do this too.
Accept
Change Settings
Cookie Box Settings
Cookie Box Settings
Privacy settings
Decide which cookies you want to allow.You can change these settings at any time. However, this can result in some functions no longer being available. For information on deleting the cookies, please consult your browser’s help function.Learn more about the cookies we use.
With the slider, you can enable or disable different types of cookies:
This website will:
Remember which cookies group you accepted
This website won't:
Remember your login details
Essential: Remember your cookie permission setting
Essential: Allow session cookies
Essential: Gather information you input into a contact forms newsletter and other forms across all pages
Essential: Keep track of what you input in a shopping cart
Essential: Authenticate that you are logged into your user account
Essential: Remember language version you selected
Functionality: Remember social media settings
Functionality: Remember selected region and country
Analytics: Keep track of your visited pages and interaction taken
Analytics: Keep track about your location and region based on your IP number
Analytics: Keep track of the time spent on each page
Analytics: Increase the data quality of the statistics functions
Advertising: Tailor information and advertising to your interests based on e.g. the content you have visited before. (Currently we do not use targeting or targeting cookies.
Advertising: Gather personally identifiable information such as name and location
This website will:
Essential: Remember your cookie permission setting
Essential: Allow session cookies
Essential: Gather information you input into a contact forms, newsletter and other forms across all pages
Essential: Keep track of what you input in a shopping cart
Essential: Authenticate that you are logged into your user account
Essential: Remember language version you selected
This website won't:
Remember your login details
Functionality: Remember social media settings
Functionality: Remember selected region and country
Analytics: Keep track of your visited pages and interaction taken
Analytics: Keep track about your location and region based on your IP number
Analytics: Keep track of the time spent on each page
Analytics: Increase the data quality of the statistics functions
Advertising: Tailor information and advertising to your interests based on e.g. the content you have visited before. (Currently we do not use targeting or targeting cookies.
Advertising: Gather personally identifiable information such as name and location
This website will:
Essential: Remember your cookie permission setting
Essential: Allow session cookies
Essential: Gather information you input into a contact forms, newsletter and other forms across all pages
Essential: Keep track of what you input in a shopping cart
Essential: Authenticate that you are logged into your user account
Essential: Remember language version you selected
Functionality: Remember social media settings
Functionality: Remember selected region and country
This website won't:
Remember your login details
Analytics: Keep track of your visited pages and interaction taken
Analytics: Keep track about your location and region based on your IP number
Analytics: Keep track of the time spent on each page
Analytics: Increase the data quality of the statistics functions
Advertising: Tailor information and advertising to your interests based on e.g. the content you have visited before. (Currently we do not use targeting or targeting cookies.
Advertising: Gather personally identifiable information such as name and location
This website will:
Essential: Remember your cookie permission setting
Essential: Allow session cookies
Essential: Gather information you input into a contact forms, newsletter and other forms across all pages
Essential: Keep track of what you input in a shopping cart
Essential: Authenticate that you are logged into your user account
Essential: Remember language version you selected
Functionality: Remember social media settingsl Functionality: Remember selected region and country
Analytics: Keep track of your visited pages and interaction taken
Analytics: Keep track about your location and region based on your IP number
Analytics: Keep track of the time spent on each page
Analytics: Increase the data quality of the statistics functions
This website won't:
Remember your login details
Advertising: Use information for tailored advertising with third parties
Advertising: Allow you to connect to social sites
Advertising: Identify device you are using
Advertising: Gather personally identifiable information such as name and location
This website will:
Essential: Remember your cookie permission setting
Essential: Allow session cookies
Essential: Gather information you input into a contact forms, newsletter and other forms across all pages
Essential: Keep track of what you input in a shopping cart
Essential: Authenticate that you are logged into your user account
Essential: Remember language version you selected
Functionality: Remember social media settingsl Functionality: Remember selected region and country
Analytics: Keep track of your visited pages and interaction taken
Analytics: Keep track about your location and region based on your IP number
Analytics: Keep track of the time spent on each page
Analytics: Increase the data quality of the statistics functions
Advertising: Use information for tailored advertising with third parties
Advertising: Allow you to connect to social sitesl Advertising: Identify device you are using
Advertising: Gather personally identifiable information such as name and location
 EN
EN FR
FR

")





")

")



")




")






{kind=link}
What a beautiful picture of Adolf Hitler.